|
GENE
MUTATIONS, MICROCIRCULATORY ABNORMALITIES, ONCOLOGICAL TERRAIN, AND
ONCOGENESIS (SECOND PART).
Oncological Terrain.
Clinical Contribution to primary Prevention of malignant Tumours.
Congenital
Acidosic Enzyme-Metabolic Histangiopathy-a (CAEMH-a).
Type
a and Type b Restano’s Manoeuvre.
Oncological
Terrain Diagnosis.
Simulated
sucking test and oncological terrain.
Biophysical-Semeiotic
Evaluation of Epiphysial Secretion of Melatonin.
Oncological
Terrain. Clinical Contribution to primary Prevention of malignant
Tumours. (Note: for
understanding the following review of the book “Il Terreno
Oncologico. Semeiotica Biofisica: Contributo Clinico alla Prevenzione
Primaria del Tumore”, accepted for publication by Minerva Medica
Edizioni, Turin (I am looking for..sponsor...any more), doctor
needs accurate and complete knowledge of Biophysical Semeotics. However,
in the interest of reader who is not jet experienced in the new method,
to facilitate him in the comprehension of paper, I provide some useful
informations [in
square parentheses], in a very easy manner from the technical point of view). Before
illustrating Clinical Microangiology of both “real risk” for
malignancies, both liquid and solid, it is necessary to describe in
details the oncological terraine or pre-oncological stage, based
on the Congenital Acidosic Enzyme-Metabolic Histangiopathy (CAEMH),
which proved to be the conditio
sine qua non of the oncological terraine in a well established
45-year-long clinical experience, and, therefore, of malignancy,
elsewhere exhaustively illustrated (See: later on and in the site). In
my opinion, in fact, to perform an efficacious cancer primary prevention
we must consider not only gene mutations, i.e., n-DNA, but particularly
alterations of m-DNA. CAEMH-a,
a congenital, functional, mythocondrial cytopathology, inherited almost
from the mother, lasts all life long, although variable in intensity, in
relation to life-style, diet and employment of
both bioactive products and histangioprotective drugs. Therefore,
we face here the first remarkable event, untill now overlooked: the
transmission of breast cancer as well as of all other tumours, even
involving male biological systems (as prostate) to offspring is
carried out almost always by mother. In fact, CAEMH-a
is almost always inherited by mother.
As
a matter of fact, recent researches supply further evidence for prostate
cancer susceptibility genes on chromosomes 14 and X, and they
highlight a new region of interest on chromosome 7, that may be involved
in the etiology of both prostate cancer and breast cancer
(35). On
the contrary, oncological terrain, originated on the basis of
CAEMH-a,
can disappear, to be caused or, finally, can increase by unfavourale
environmental conditions, by improper diet, etymologically speaking,
which acts in a negative manner on the CAEMH-a,
as well as on the biological systems controlling oncogenesis. In other
words, oncological terraine, in which CAEMH-a
plays a major role, can be induced
and fortunately reversed, almost completely, with the aid of correct
diet, etymologically speaking, and by means of histangioprotective
treatment (See later on). Biophysical
Semeiotics
allows doctor to recognize and evaluate “quantitatively” the pre-oncological
stage, i.e. oncological terrain,
by the aid of a large number of methods, different in
simplicity, refinement, practical application and amount of information. The
usefulness of all these clinical methods, in doctor’s daily work, is
pointed out by the fact that the absence of oncological terrain rules
out the presence of whatever malignancy, influencing remarkebly the
diagnostic iter, large scale screening, and therapeutic
monitoring. In
fact, age, sex, familiarity have now , i.e. from biophysical
semeiotic point of view, a very little value in oncological prevention,
because exclusively clinical recognition of oncological terrain requires
urgently that patient undergoes to instrumental and sophisticated
semeiotics, early, in a rational manner, after ascertaining the type II
microcirculatory activation, non-associated [=
pathological preconditioning]
even in a small part of well defined biological system, where preconditioning
results pathological, besides to other numerous biophysical
semeiotic signs (See: Early Diagnosis of Heart .... in Home-Page). In
each human there are about 1013 cells: not all of these cells,
but almost all, can grow and replicate to present as a clinical cancer
in every time, due mutations occuring during cellular reproduction.
However, cancer is a rare disease at the cellular level. As a
matter of facts, up to 30% of all individuals in the developed countries
will present clinically with one of a wide variety
of cancer at some time of their life. Consequently,
if the number of cell at risk is taken into account, given the relatively
small cases of malignancies, it is obvious that this disease only
rarely escapes normal protective systems. Therefore, tumours can
originate and grow exclusively when psycho-neuro-endocrine-immunological
system is profoundly modified. As regards both primary prevention and
clinical diagnosis of malignancy, in my opinion, answering to the
following question is essential:
“What does carachterize oncological terrain from the clinical
view-point?”. In
fact, in order to achieve efficacious prevention on large scale
it is unavoidable that all the modifications occurring in the biological
controll system could be easily and promptly ascertained and properly
evaluated with the aid of clinical method, i.e. by the use of a
sthetoscope, and certainly without application of sophysticated
semeiotics, that does not apply in all individuals, and, moreover, only
a few doctors can utilize them. If
it is possible answering affirmatively to this question, a second one
immediately follows: “The
oncological terrain, which certanly can be induced, is also in some way
reversible?” It
is urgent and necessary to know if
the oncological terrain can be reversed, i.e. it can
totally or greatly disappeare, with the aid of drugs or diet,
etymologically speaking, which exert a favourable influence on
modifications of the psicho-neuro-endocrine-immunological system, caused
always by m-DNA alterations . Congenital
Acidosic Enzyme-Metabolic Histangiopathy-a
(CAEMH-a).
At
first, we must both face and resolve essential problems concerning
oncological terrain, discussing, once again,
accurately the pathological mitochondrial condition, which
represents its fundamental basis, when it is particularly severe: CAEMH-a.
(See Congenital Acidosic Enzymo-Metabolic Histangiopaty in the site) CAEM-a,
conditio sine qua non also of oncological terraine, represents
actually a severe alteration of mitochondrial oxidative phosphorilation
processes, i.e. ATP synthesis, as well as nucleophyl substitution,
variable in intensity from individual to individual, from tissue to
tissue and from part to part of the same tissue. From
morphological point of view, it is well-known that CAEM-a
is characterized by prevalence of right cerebral hemisphere – right
cerebral dominance – or more correctly said, of right Planum
temporale, which is notoriously located between Heschl’s
convolution (gyrus) and posterior part of Silvio’s fissure. One
can ascertain CAEM-a
as elsewhere described (See Bibliography in the site). However, it is
advisable an easiest manner, briefly illustrated in following: in
healthy individual in supine position and psycho-physically relaxed,
doctor applies its left hand, at first, on right parietal-temporal
region of the subject and then on the left one, when the individual to
be examined presses forefinger-pulp and thumb-pulp together, obviously
at first, of the left hand and, subsequently, of the right one; at the
same time doctor evaluate somatosensorial evoked potentials (SEPs)
[=
in pratice, latency time of the cerebral-gastric aspecific reflex, as
indicated in Fig. 1]. In
case of CAEMH-a,
latency time (lt) of the
reflex is 6 sec. when trigger-points of right hemisphere are stimulated,
whereas lt results 7 sec. if left cerebral trigger-points are
activated; in later situation, intensity of gastric aspecific reflex
appears clearly lower: 2 cm versus 1 cm. respectively.
Of course, the degrees of reflex intensity are reversed in
presence of dominance of left cerebral hemisphere. At
this point, in order to observe the interesting evolution from CAEMH-a
to oncological terrain, one must remember, once a time, an
usefull biophysical semeiotic syndrome, really helpful to general
pracitioner in everiday activity: the Rethyculo-Endothelial System
Hyperfunction Syndrome (RESHS),
that is subdivided in three types: “complete”, “intermediate”
and “uncomplete” type. As
far as clinical significance is concerned, CAEMH-a
corresponds to ESR elevation and proteins electrophoresis alterations,
but surely is of both more sensitive, specific and, therefore, reliable.
In fact, in case of a slight attack of flu, e.g., (or, even, in advanced
cancer) it often turns out
that both laboratory tests are in normal ranges, while RESHS “uncomplete”,
carachteristic of this viral disease, is always present since the first,
asymptomatic stage, when evaluated by aid of the Restano’s
maneouvre [=
patient clinches fists and does not breath, i.e. boxer’s and
simultaneously apnea test: sympathetic hypertonus]
(See: Glossary in Home-Page): in healthy young person, psycho-physically
relaxed, in supine position, digital pressure of “mean” intensity,
applied on mean line of breast-bone, iliac crests and spleen projection
area, provokes the gastric aspecific reflex after a latency time of 10
sec.: RESHS physiological
(Fig.8). In
case of bacterial infection, contagious diseases of infancy, viral
in origin, connective tissue disorders (Rheumatoid Arthritis, Lupus
Erithematosus, a.s.o.), malignant tumours, a.s.o., lt decreases to 6
sec. with a latency time of reinforcing [=
augmentation of reflex intensity]
of 8 ±
1 sec.:
RESHS “complete”. On
the contrary, in viral flu, as in commom flu, digital pressure, applied
on cutaneous projection area of spleen does not brings
about any gastric aspecific reflex, because white germ centres of
splenic (red) pulp are not activated in these conditions: RESHS “uncomplete”.
On the contrary, in Herpes Zoster as well as in common infectious
diseases of infancy, caused by viral, RESHS is “complete”. Finally,
in bacterial disorders, provoked by Gram-negative, i.e. in common acute
cystitis (E.coli) or
in antritis brought about by H. pylori, RESHS turns out to be
“intermediate” (Tab.1).
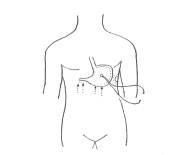
Fig.
8 Reticulo-Endothelial
System Hyperfunction Syndrome: in
the stomach, both fundus and body are clearly dilated, while
antral-pyloric region contracts
(= gastric aspecific reflex), when digital pressure of mean intensity is
applied on middle line of breast-bone, iliac crests and, only in the
“complete” type, also on cutaneous projection area of the spleen,
after a latency time less than 10 sec. (NN = 10 sec.) (See text and Tab
1).
RESHS:
types and clinical significances.
Tab.
1 Interestingly, RESHS
allows doctor to monitoring in objective manner the course of wathever
disorder in objective manner. As a matter of facts, the degree of both lt and
lt of reflex reinforcing provides essential information about the course of
the underlying illness. From
the practical view-point, it is of interest that exclusively during the
changing of RESHES, from “uncomplete” to “complete” type, doctor has
to prescribe immediatly, without delay, antibiotic drugs. A
long, well-established experience, allows
me to state that doctor recognizes easily, with the aid of
Biophysical Semeiotics, individuals CAEMH-a-positive at oncological risk, quantifying it and, therefore, estimating the
probability of tumour. Type
a and Type b Restano’s
Manoeuvre. In
85 % of malignant tumours, both solid and liquid, in initial stage and in
100 % when malignancy is already advanced, RESHS is of “complete” type,
showing a characteristic latency time (lt) of only 3 sec. and
latency time of reinforcing of 5,5 ±
0,5 sec. By
contrast, in common viral diseases of infancy and in bacterial disorders,
connectivitis, a.s.o., lt is 6 sec. and latency time of reinforcing
is 8,5±0,5
sec.; p <0,001.
In
patients, succesfully operated of malignant tumour, lt is 10 sec.
(NN = 10 sec.), but after apnea test, lasting 10 sec. and boxer’
tests, employed simultaneously, i.e. Restano’s manoeuvre, lt
is lower (3 sec.) and lt of reinforcing turns out to be 8 ±
1 sec.
(Tab.1 and 2 ). Interstingly,
in healthy without positive familiarity for tumours, Restano’s
manoeuvre brings about only a small modification of basal lt and lt of
reinforcing is 9,5 ±
0,5 sec. Finally,
it is of great interest that in both initial stage of tumours in 15 % of
cases and patients at risk of cancer, basal value oscillate in
normal ranges, but it becomes plainly pathological after Restano’s
manoeuvre, obviously with different degree (Tab. 3) (in parentheses basal values)
Tab.
3
At this point doctor must remember the essential role Restano’s
manoeuvre plays in moving from
CAEMH-a
syndrome to cancer growing. Restano’s manoeuvre represents,
indeed, the activation of Reticulo-Endothelial-System, at the present
termed Monocyte-Macrophage System. As indicates Tab. 3, there are two type
of this manoeuvre: type A and type B. In
order to observe and to evaluate “quantitatively” the manoeuvre,
subject to be examined is invited not to breath for 10 sec. (apnea test),
or alternatively doctor applies intense, occlusive digital pressure on a
brachial artery for the same time (10 sec.), i.e. “variant” Restano’s
manoeuvre, as well as to clinching fists: sympathetic hypertonus. Before
the individual keep again to normally breath, doctor applies digital
pressure on middle line of
breast-bone (or on iliac crests or cutaneous prjection area of the spleen)
for evaluating RESHS [=
lt of gastric aspecific reflex, i.e. fundus and body of the stomach
appear dilated, while antral-pyloric region contracts, and lt of reflex reinforcing]
(Tab. 1). As
described-above, Restano’s manoeuvre points out RESHS activation.
As a matter of facts, e.g. during infectious disorder, it appears earlier
type A, then type B and finally RESHS, “complete”,
“uncomplete” or “intermediate”, in relation to the nature od
underlying disese. On
the other hand, when therapy ameliorates the underlying disorder and
patient improves, first of all RESHS disappears, and therafter also type B
of the manoeuvre is not ascertained, while appears type A , which lasts as
far as patient completely recovers.
The
presence of Restano’s manoeuvre type B, i.e. the activation of
Reticulo-Endothelial System, is due to the fact that marrow products
mononuclear cells, which migrate to the thymus and lymphoid tissues, as
well as myelopeptides, that stimulate antibodies synthesis, in order to
increase biological defense. Consequently, there is marrow
microcirculatory activation type I, associated [=
“light” digital pressure on breast-bone, e.g.,
provokes three ureteral reflexes, which permit doctor to evaluate
vasomotility and vasomotion of marrow microcirculation, by the intensity
of reflexes fluctuation]. Following
experimental evidence corroborates my above-illustrated interpretation: in
healthy individual, “intense” digital pressure on trigger-points to
evaluate RESHS (middle line of breast-bone, iliac crests) after about 20
sec. increases the antibodies biophysical semeiotic syndrome [=
light digital pressur, applied on MALT skin projection, i.e. breast-,
liver-, spleen-, urinary bladder-, appendix-, middle clavicular
line- a.s.o., cutaneous projection areas, provokes physiologically
after 6 sec. gastric aspecific reflex of 2 cm. in intensity:
chronic antibodies synthesis syndrome],
that from the chronic type becomes
clearly of acute type, where lt appears to be 3 sec. and
intensity > 2 cm. On
the contrary, in individual with oncological terrain stimulation of
antibodies synthesis appears to be whether absent or not statistically
significant (lt of MALT-gastric aspecific reflex: 5-6 sec.). Moreover, in
healthy, digital pressure on middle line of breast-bone, after a lt of
about 20 sec., increases the diameters of BALT cutaneous projection area
(
3 cm.), while in oncological
terrain they increase only £
1 cm. [=
auscultatory percussion of both posterior and anterior thoracic wall,
allows doctor to ascertained , along middle scapular and, respectively,
clavicular line, three round hypophonetic area – BALT – of a diameter
oscillating in a chaotic-deterministic manner, 6 times/min, from
0,5 cm. to 1,5 cm., with a period varying from 9 sec. to
12 sec., mean value 10,5, a fractal number,
as do all biological systems]. Interestingly,
in healthy individual digital pressure of mean intensity, applied on
breast-bone provokes, after about 20 sec.,
intense increasing (³
2 cm.) of
BALT cutaneous projection areas, with augmentation of antibodies synthesis
[=
lt of MALT-gastric aspecific reflex lowers from 6sec.to 3 sec. and reflex
intensity clearly increases to ³
2 cm.],
while in presence of oncological terrain the encreases is
£
1 cm.). To
demonstrate both internal and external coherence of biophysical theory it
is whortwhile that simultaneously, during Restano’s manoeuvre,
all sites of antibodies synthesis (MALT) show biophysical semeiotic
features of active hyperemia, more precisely speaking, the
microcirculatory activation type I, associated (See earlier), of
course of different intensity in relation to causal agent, indicating the
acute phase of antibodies production. Notably,
the following clinical evidence corroborates this interpretation: in
healthy, subcutaneous injection of desensitizing vaccine, according to
Besredka, induces first the type A, later type B and finally RESHS. While
in Restano’s manoeuvre type A is always contemporaneously present
Selye’s syndrome, variable in intensity, beside type B doctor observe
characteristic modifications of psycho-neuro-endocrine-immunological
system, as in malignancy, liquid or solid, as well as in patients, who
successfully underwent to surgery. I have termed this pathological situation of
biological systems for protecting against cancer as “oncological
terrain”. As
regards the evaluation of neuro-stimulatotors, neuro-modulators, hormonal
neuro-modulators, free-oxygen-radicals, and preconditioning see
Bibliography in Home-Page. Oncological
Terrain Diagnosis. Biophysical
Semeiotics
allows doctor to both recognize and “quantify” at the bed-side the
biological terrain, conditio sine qua non for cancer initiating and
growing (oncogenesis) (Tab.4 and 5). Oncological terrain
ONCOLOGICAL
TERRAIN: DIAGNOSIS
AND QUANTITATIVE EVALUATION
Tab.5 However,
I describe a method, easy to perform, reliable in detecting the presence
of oncological terrain, as follows: A)
in healthy, supine and psycho-physically relaxed, during rythmic palpation
of breast (similuated sucking test, SST) the mammary
gland-gastric-aspecific reflex lasts 7 sec. exactly. On
the contrary, in oncological terrain the duration augments to 8-9 sec.
(p < 0,01) due to prolactin increasing. One must observe, however, that
even during an infectious disease, like flu, prolactin secretion increases. In
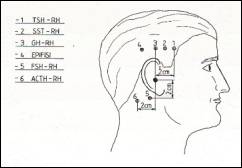
addition, digital pressure, applied 2 cm above external acoustic meatus
(Fig.9) [=
cutaneous projection area of GH-RH
neuronal center],
physiologically gastric aspecific reflex, during SST,
continues for < 10 sec., while in case of oncological
terrain is ³
10 sec. in
relation to the degree of hormonal dysfunction. In
fact, in such condition there is a loss of balance as regards restraining
and stimulating substances acting on prolactine secretion (hormons,
neuro-transmitters, a.s.o.) in favour of the later ones. Actually, SST,
easy to perform in a few seconds, plays a primary role in detecting
complicated modifications in biological systems that defend humans against
cancers. B)
In healthy, in whom basal value of SST is 7 sec. exactly,
digital pressure of mean-high intensity on mandibular nerve lasting 30
sec., induces endogenous opiates secretion, whereas lowers duration
of gastric aspecific reflex during SST to £
6 sec. (NN =
7 sec.). On
the contrary, apnea test (10 sec.), by means of sympathetic activation and
subsequent adrenaline and nor-adrenaline secretion, brings about the SST
to 12 sec. In
presence of oncological terrain, because of hormonal levels and
neurotransmettitors modifications, gastric aspecific reflex during SST,
lasts more than 12 sec., due to severe reduction of
endogenous opiates as well as somatostatine, and consequently prolactin
clearly increases. From
the above remarks, Biophysical Semeiotics permits doctor to
corroborate at the bed-side the relation between immunological process and
psycho-neuro-endocrinological, I illustrated clinically in earlier
articles (See: Oncological Terrain in the site). There
are other numerous methods, both rapid and easy to perform at the bed-side,
to estimate in reliable manner the presence and intensity of oncological
terrain, apart from the “direct” evaluation of GH-RH, ACTH-RH, SST-RH
and melatonin-secretion, apart from the “quantitative” assessment of
endogenous opiates, resulting an easy diagnosis, useful for large
scale screening. In
following, some very practical methods for evaluating oncological terrain
are briefly described : 1)
Firstly, doctor evaluates the dimension of cutaneous projection
area of one BALT site (e.g., BALT in posterior apical pulmonary location);
than, he invites the patient to close intensively both eyes, in order to avoid the light
vision (= melatonin secretion). After 5 sec. or more, of course, in
healthy, the same cutaneous
area clearly increases its diameters, in direct relation to the intensity
of melatonin secretion: normally diameter
doubles, reaching the value of 6 cm. (NN basal value = 3 cm.),
whereas in oncological terrain augments slightly: £
1 cm. Moreover,
in healthy, interestingly the duration of the same event lasts 30 sec.
exactly. On the contrary, in case of oncological terrain duration results <
30 sec., in relation to oncological risk intensity. 2)
Analogously, BALT-gastric aspecific-reflex physiologically shows a lt of 6
sec. (chronic antibodies synthesis), but it lowers to only 3
sec. after closing both eyes (5 sec. therafter) wiht an intensity
greater than that of basal one. On the contrary, in case of oncological
terrain lt as well as intensity of the reflex appears modified in a small
manner, in inverse relation to the seriousness of
disorder (= melatonin secretion). 3)
In healthy, apnea test, lasting
for about 10 sec., reduces of 1/3 diameter o cutaneous projection
area of a BALT site, whereas in patient involved by oncological terrain
the lowering reaches 2/3 or less.
Simulated
sucking test and oncological terrain. The
assessment of oncological terrain by means of
both Simulated Sucking Test (SST) and simultaneous breast
preconditioning give
doctors interesting and quantitative information on breast cancer “real
risk”: one evaluates basal duration of SST, i.e. during rhytmic
palpation of a mammalian gland, doctor estimates also the duration of
breast-gastric aspecific reflex, (NN = 7 sec. exactly). After
precisely 5 sec., doctor performes again – a second time – the
identical manoeuvre. In
healthy, the duration decreases by degrees to 6 sec and 5 sec,
respectively, since dopaminergic tone
of diencephalo-hypophysial axis physiologically increases. On
the contrary, in oncological terrain the duration rises, first to 8 sec.
and finally to ³
12 sec. Notoriously,
in both these conditions and in malignant tumours, the dopaminergic tone
of diencephalo-hypophysial axis appears reduced and consequently prolactin
secretion augments. Therefore, the diagnostic value of SST and breast preconditioning is of
paramount importance in both ascertaining oncological terrain and
diagnosing malignancy. As
a matter of facts, in malignant cancers, solid as well as liquid, basal SST persists for ³
10 sec. (NN
= 7 sec.) identical value is observed in initial stages of cancer, in
patients who successfully underwent surgery
and, finally, in individual at real risk of tumour, i.e.
with oncological terrain. Before
65 years, SST is
neither age- nor sex-dipendent
(NN = 7 sed. exactly). After
apnea test lasting about 10 sec. (= patient does not take any breath), in
oncological terrain, SST
increases from 12 to 20 sec. pathologically (NN = 10 sec.
precisely), so that basal SST
of 12 sec. in individual under 65 years of age indicates by it-self
a pathological condition of activated immunological system. It
is of interest that the from CAEMH (=Congenital Acidosic
Enzymo-Metabolic Histangiopathy) to Restano’s manoeuvre typ A and,
then, type B, of variable intensity, indicating the presence of
oncological terrain, the passage is both slow and gradual. A
long, well established experience allows me to state that normocaloric,
correct diet and physiological
life-style, as indicated in the
decalogue of European Society for Study and Prevention of Cancer and,
finally, the use of histangioprotective drugs (Co Q10,
Carnetine, Vit A and E, Bioflavonoidds, Capsaicin, a.s.o.)
cause oncological terrain disappearing.
Interestingly,
such as knowledge is useful for patient, doctor and NHS. On the contrary,
in presence of modifications of psycho-neuro-endocrine-immunonogical
system, doctor must exclude the tumour, even in early stage, evaluating
the real risk in well-localized tissue. Soon
thereafter, both efficacious therapy and correct diet, ethimologically
speaking, in order to bring about the normalisation of all altered
parameters, relating to SST, GH, IGfs, endogenous opiates, free
Radicals, antioxidants, Co Q10, hyperinsulinemia-insulin resistance and
melatonin, must be prescribed and their action monitored. Biophysical-Semeiotic
Evaluation of Epiphysial Secretion of Melatonin. For
the first time, doctor can evaluate “clinically” by means of Biophysical
Semeiotics the epiphysial secretion of melatonin,
N-acetyl-5-methoxy-triptamin, which notoriously stimulates the antibody
synthesis, activating opiates receptors, i.e. indirectly, as well as
inhibits both normal and neoplatic cells growing.
Fig.
9 Numerous
biophysical semeiotic methods allow doctor to assess melatonin level at
the bed-side in easy and reliable manner: 1)
in healthy, whose eyes are closed since 5 sec. or more, antibodies
synthesis appears clearly enhanced: for instance,
BALT cutaneous projection area shows its diameters doubled and
simultaneously peristaltic waves velocity, e.g. in the stomach, results
clearly slower, because it needs ³
12 sec. (NN
= 5 sec.) for reaching antral-pyloric
region, starting from initial part of the fundus [=
ascertained cutaneous projection of the great gastric curvature, doctor
gives a pinch to the skin covering breast-bone, ensiform appendix:
immediately a peristaltic wave originates, which physiologically reaches
antral-pyloric region in 5 sec. exactly].
These modifications last for 30 sec. precisely, i.e. their duration
results identical to that of melatonin secretion under the same condition
(eyes closed) (See later on); 2)
mean-intense digital pressure, applied on epiphysial cutaneous
projection area, i.e. 2 cm above and 2 cm posteriorly external acoustic
meatus (Fig. 9), after about 5 sec. provokes the same biophysical
semeiotic signs, above described at point 1), which show identical
duration, proving clearly internal as well as external coherence of the
theory; 3)
in healthy, intense digital pressure, applied on mandibular branch of nervus
trigeminus (trigeminal nerve), starting from ³
15 sec. brings about endogenous opiates increasing, epiphysial
microcirculatory activation type I, associated [=
during small digital pressure on epiphisyal neuronal center
ureteral reflexes fluctuate in an intense manner(HS) with fixed
periods of 10 sec.],
enhancement of antibodie synthesis (“acute type”: lt BALT-gastric
aspecific reflex is 3 sec.) and simoultaneously peristaltic wave slows
down: the time necessary
to a wave, originated in initial segment of fundus, for
reaching antral-pyloric region, from
5 sec. rises to ³
12 sec. In
oncological terrain melatonin secretion results evidently altered, of
variable degree from individual to individual, of course, easy to
ascertain by the aid of above-illustrated parameters. Interestingly,
a clinical evidence suggests that epiphysial activity
is evaluated in a rapid and reliable manner by means of Biophysical
Semeiotics: in healthy, stimulating endogenous opiates secretion, with
the aid of intense digital pressure on mandibular nerve, the peristaltic
wave in the stomach slows down so far that it needs
³
12 sec. (NN
= 5 sec precisely) for reaching antral-pyloric region. At the same time,
intensity of cerebral-gastric aspecific reflex during the evaluation of
cerebral evoked potentials [=
patient, in supine position and relaxed, push two finger-pulps against
each other, while doctor estimates lt of cerebral gastric aspecific reflex
on right, and then, on links hemisphere: in health, lt is 6 sec.
and 7 sec. respectively with intensity of 2,5 cm.]
decreases from normal value of 2,5 cm. to < 2 cm. If
these parameters, however, are evaluated in healthy individual with closed
eyes, during the application
of intense digital pressure on epiphysial cutaneous projection area for 30
sec. (Fig.9), doctor observes clear modifications of parameters value: lt ³
10 sec. and <
1,5 cm respectively. This
experimental evidence suggests that melatonin, secreted under such as
condition, acts directly as well as indirectly by means of endogenous
opiates, of which action, therefore, results more efficacious, allowing
thus a “quantitative” assessment of actual level of
N-acethyl-5-methoxy-tryptamin. In
addition, clinical evidence demonstrates that melatonin, when associated
whith endogenous opiates, stimulates more intensively
acute antibody synthesis. To
summarize,
in daily practice, to ascertain oncological terrain, in complete,
qualitative as well as quantitative manner, it appears advisable the
diagnostic iter, easy and reliable, described as follows: 1)
evaluation of basal peristaltic wave velocity (NN = 5 sec.);
2) evaluation of GH secretion by mean of the stimulation of its
cutaneous prjection area, i.e. GH-RH neuronal centre skin projection
(Fig.9), localized 2 cm above external acoustic meatus: in healthy,
duration of splenic congestion (enlargment of spleen) is 6 sec.,
whereas splenic decongestion lasts 20 sec. precisely. Moreover,
during this manoeuvre, doctor estimates also the time necessary to
peristaltic gastric wave (even when it is caused by pinching
the skin of Hiss angle cutaneous projection area) to reach
antral-pyloric region moving along gastric great curve: ³
12 sec. (NN
= 5 sec.), because GH stimulates somatostatin secretion, that slow down
gastro-intestinal peristalsis and bring about decongestion of the
splanchnic territory. Starting
from 20-25 sec of GH-RH stimulation, evaluated above mentioned parameters,
stopped the manoeuvre, immediately doctor estimates SST duration,
whis physiologically is < 10
sec., due to the fact that valid secretion of somatostatin as well
as physiological level of dopamine in diencephalo-hypophysial axis
restrain the prolactin secretion, induced by GH. In
fact, both substances influence negatively prolactin secretion. At
the end of the stimulation of
GH-RH secretion (and of all other RH secretions, of course) in healthy
pancreas augments its diameters
(practically, pancreatic inferior border lowers due to congestion for
exactly 8 sec. Interstingly, this value is fundamental in
diagnosing alterations of glucose metabolism or insulin-secretion. In
fact, in case of diabetes mellitus the duration of inferior
pancreatic margin lowering amounts to < 8 sec. (NN = 8 sec.), in
direct relation to severity of the syndrome. On
the contrary, in both IGT and
hyperinsulinemia-insulinresistance the pancreatic enlargement lasts
for > 8 sec., once again in correlation with the increas of
hormonal secretion, showing the
possibility of evaluating simultaneously different disorders by
means of Biophysical Semeiotics, since the numerous biological
systems are connetted very closely from both structural and functional
point of view. At
this point, oncological terrain is recognized and can be
“quantitatively” evaluated in
other manners, as follows: 3)
assessment of endogenous opiates, the so-called “immunological orchestra
directors”; 4)
estimation of melatonin level, as described above. As
far as the evaluation of endogenous opiates system concerns, that can be
activated also by melatonin and myelopeptides, a refined method is
represented by assessment of cerebral-gastric aspecific reflex intensity,
first, at basal line (NN 2-3
cm.) and, then, after intense
digital pressure on mandibular nerve for 25 sec., during Cerebral Evoked
Potentials (See earlier): in healthy, intensity of cerebral gastric
aspecific reflex is reduced to a half., due to the restraining action of endogeous opiates as regards the neurotransmission. In
oncological terrain, characterized by the typical lack of
b-endorphins
as well as met-enkephalin, above-mentioned stimulation of endogenous
opiates provokes a very small decreasing of cerebral-gastric aspecific
reflex. To
summarize,
one method, easy and rapid to perform, reliable in both diagnosing and
“quantitatively” evaluating oncological terrain, in my opinion, is the
following: closing eyes enhance melatonin
epiphysial secretion, constantly reduced in oncological terrain, obviously
whith different degree. Notoriously, melatonin stimulates
diencephalo-hypophysial secretion of SST-RH as well as of
endogenous opiates, particularly in arcuate nucleus. In addition,
melatonin, somatostatin, and particularly endogenous opiates stimulate
antibody synthesis. Consequently,
BALT cutaneous projection area, evaluated
at rest and after 5 sec. eyes closure (patient closes intensively
his eyes) appears clearly modified and doubled in healthy for 30 sec.,
whereas in oncological terrain, in relation to its intensity, changes are
minimal (£
1 cm.) for < 30 sec. in relation to the severity of
underlying abnormality of psycho-neuro-endocrine-immunological system.
Really, the test end is immediately followed by transitory enlargement of
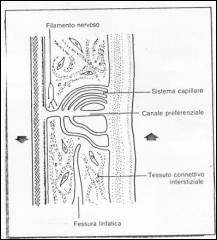
BALT size, easy to detect. When
CAEM-a,
if particularly intense, involves both parechymas and related mivrovessels
of various sytems, underlying psycho-neuro-endocrine-immunological system,
it provokes oncological terrain. In such as situation, as reader knows it,
there are structural as well as functional microcircolatory abnormalities,
even localised in well defined tissues or parts of tissue, i.e. the
phenomenon of “blood-flow centralization”, which brings about
subsequently parenchymal disorders (Fig. 10).
Fig. 10 Explanation
in the text. This
pathological microcirculatory condition, genetically inherited, and
related to CAEMH-a,
“caan” cause degenerative parenchymal diseases (dyslipidemias,
diabetes mellitus, ATS, arterial hypertension, a.s.o.) under the negative
influences of well-known environmental risk factors
(See in above cited site: “Biophysical_Semeiotic Constitutions”). Oncological
terrain by it-self, however, can not cause oncogenesis, as the
“sole” presence of gene mutations of n-DNA can not provoke cancer
onset. Infact, gene mutations brings about not always cancer onset, at the
most the inititiation only. I
think (conjecture) that gene mutations of nuclear DNA, at the most, can
provoke cell oncological initiation, but not oncological progression: the
body’s efficacious defense reaction, thanks to physiologically
functioning PNEI system, can successfully destroy degenerated cell or
repair it. In
conclusion, gene mutations of DNA involve, by isolated or combined way,
both mitochondrial DNA, which “can” cause oncological terrain, and
nuclear DNA, ending to well-known mutations. In
case of isoleted gene mutations, it is possible the onset – mDNA
abnormality – of most severe and common human diseases, except for
cancer, and, under the later condition – nDNA abnormality – the single
cancer initiation, followed by either degenerated
cell destroyng or its recovery to a “social” element.
To
summarize, genetic factors underlying the most severe and common
human diseases are represented by mitochondrial
and nuclear abnormalities. The first are inhereted almost always throug
the mother and “can” provoke oncological terrain, originating CAEM-a. However,
when “isolated”, i.e. not associated with nuclear DNA gene mutations,
they “can”, if intense, cause degenerative-metabolic disorders, in
different ways associated each others in a single patient, but they can
not bring about malignancy onset, independently
of their severity. Analogously,
nuclear genetic factors, i.e., the well-known gene mutation of
nuclear DNA, if single, namely dissociated from m-DNA abnormalities,
“can not” provoke the above-mentioned diseases, including cancer: at
the most, in particularly severe cases, it is possible cancer initiation,
which does not progress to cancer in the absence of oncological terrain;
degenerated cell is immediately either destroyed or transformed in a
“social” cell by repairing. Malignancy,
therefore, according to my conjecture, “can” initiate and progress
only when are associated both DNA alterations, mitochondrial and nuclear:
the firsts provoke functional and structural abnormalities of
tissue-microvascula-unit (for instance, behavioural abnormality
during inculin secretion acute pick test), whereas the
seconds probably aggraviate structutral alterations of local
microvessels and/or abnormal microvessel responses to different stimuli,
physiological and pathological. In
conclusion, malignancy initiates and progresses in presence not only of
nuclear gene mutations, as clinical evidence shows, but also in presence
of alterations, genetically caused, of mithocondrial DNA, conditio sine
qua non of oncogenesis and all other severe disorders, as I
emphasized since three decades (36, 37, 38) (See my site). Interestingly,
in initial stage, “in situ” evaluation of ureteral trajectories,
described above, basal as well as after stimulation, e.g., of GH by means
of digital pressure applied on cutaneousprojection area of this neuronal
centre lasting 20 sec. (See Oncological Terrain). Infact, vasomotion
parameters result intensively pathological, due to growth factors induced
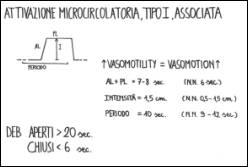
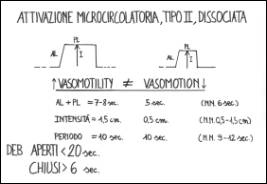
by GH. In
healthy, the test provokes interesting microcirculatory modifications:
both vasomotility and vasomotion appear more intense, showing a AL + PL
phase increased to 7 sec., due to type I microcirculatory
activation, at the level of prostate histangium: increasing of
local histangic O2 (=
latency time of gastric aspecific reflex isgreater than basal value). By
contrast, in individual involved by “real oncological risk”, in those
with “in situ” cancer or, of course, when cancer has already
progressed, independently of severity, GH-induced microcirculatory
activation I is dissociated, or of type II, and doctor observes intense
oscillation like Highest Spike, showing 1,5 cm. Intensity, in the
sole vasomotility (= upper ureteral reflex), with AL + PL phase of 8
sec., whereas analogue and subsequent vasomotility fluctations (=
lower ureteral reflex) show lowest intensity (0,5 cm.), with AL + PL phase
of only 5 sec. and EBD particularly “closed”:consequently, a
severe pH lowering, causing the particular pathological behaviour of
reflexes (Fig. 11, 12). .
Fig. 11
Fig.12 As
GH, acute pick test of insulin secretion brings about a pathologica
microvascula reaction at the level of prostate area at real risk of cancer,
or, of course, already involved by malignancy. As
a consequence, such as endogenous insulin test proved to be really useful
in early diagnosing as well as in the prostate cancer staging, in a long
clinical experience. Between
these two extreme events related to microcirculatory activation, GH- and
insulin-induced, there are a lot of “intermediate” stages, where
vasomotility increased activity successfully supply
a basal normal capillary blood-flow to parenchyma: vasomotion AL +
PL of 6 sec. In
conclusion,
in a 50 year old subject, the observation of biophysical-semeiotic data,
e.g., of prostate cancer and particularly Massucco’s
sign (Glossary), allow doctor
to diagnose prostate cancer. At
this point, we analyse, for instance, the contribution of Biophysical
Semeiotics to prostate cancer “clinical” staging. First of
all, the site can be uni- or bi-lateral, if prostatic
trigger-point stimulation shows positive results uni- or
bi-laterally. Secondly,
when “interne” prostate is involved, also local trigger-points
stimulation (= I lumbar dermatomere: in practice, groin skin) provokes
pathological signs. One must remember that the possible presence of calcification
is revealed by typical “lithiasic” reflex: prostate related
trigger-points stimulation provokes “in toto” ureteral reflex, that
rapidly reaches its highest value, and then reduces by a third exactly. When
there is tpe II, dissociated, microcirculatory activation, with intense
vasomotility, and vasomotion is slight or not at all altered, pH not
particularly lowered (reflex latency time > 6 sec.), including Massucco’s
sign, cancer severity is reduced. On
the contrary, microcirculatory “failure”, involving prostate entirely,
shows highest malignancy. Finally,
antibody synthesis evaluation at the level of local MALT appears to be
very usefull: digital pressure upon lower and internal area of iliac
fossa, at links and right ( site of prostate lymphonodes) brings about
acute antibody syndrome (gastric aspecific latency time 3 sec.), and
gastric aspecific lt, its duration, and tonic Gastric
ontraction parallel the
intensity of the underlying syndrome.
References. 1) Watts G. Three cell cycle scientists win Nobel prize. BMJ 2001; 323:823 (13 October). 2) Stagnaro-Neri M., Stagnaro S., Semeiotica Biofisica del torace, della circolazione ematica e dell’anticorpopoiesi acuta e cronica. Acta Med. Medit. 13, 25 1997 3) Stagnaro-Neri M., Stagnaro S., Semeiotica Biofisica: la manovra di Ferrero-Marigo nella diagnosi clinica della iperinsulinemia-insulino resistenza. Acta Med. Medit. 13, 125 1997 4) Stagnaro-Neri
M., Stagnaro S., Cancro della mammella: prevenzione primaria e diagnosi
precoce con la percussione ascoltata. Gazz. Med. It. – Arch.
Sc. Med. 152, 447,
1993. 5)
Stagnaro S., Diet and Risk of Type 2 Diabetes. N Engl J Med. 2002 Jan 24;346(4):297-298. letter [PubMed
–indexed for MEDLINE]. 6) Cortez D, Wang Y, Qin
J, Elledge SJ. Requirement
of ATM-dependent phosphorylation of brca1 in the DNA damage response to
double-strand breaks. Science 1999;286:1162-6. 7)
Li S, Ting NSY, Zheng L, et al. Functionallink ofBRCA1 and ataxia
telangiectasia gene product in DNA damage response. Nature 2000;406:
210-5. 8)
Bell DW, Vatley JM, Szydlo TE, et al. Heterozygous germ line hCHK2
mutations in Li-Fraumeni syndrome. Science
1999;286:2528-31. 9)
Hirao, A, Kong, Y-Y, Matsuoka S, et al. DNA damage-induced activa- tion ofp53 by the checkpoint kinase Chk2.
Science 2000;287:1824-7. 10)
Zhao S, Weng Y-C, Yuan S-S, et al. Functionallink between ataxia-tel-
angiectasia and Nijmegen breakage syndrome gene products. Nature 2000;
405:473-7. 11)
Wu X, Ranganathan V, Weisman DS, et al. ATM phosphorylation of Nijmegen
breakage syndrome protein is reqnired in a DNA damage response. Nature
2000;405:477-82. 12)
Lee J-S, Collins KM, Brown AL, Lee C-H, Chung JH. hCds1-Mediated
phosphorylation of BRCA1 regulates the DNA damage response. Nature
2000;404:201-4. 13)
Wang Y, Cortez D, Yazdi P, NeffN, Elledge SJ, Qin J. BASC, a super complex
of BRCA1-associated proteins involved in the recognition and repair of
aberrant DNA structures. Genes Dev 2000;14:927-39. 14)
Swift M, Morrell D, Massey RB, Chase CL. Incidence of cancer in 161
families affected by ataxia-telangiectasia. N Engl J Med 1991;325:1831-6. 15)
FitzGerald MG, Bean JM, Hegde SR, et al. Heterozygous
ATM mutations do not contribute to early onset of breast cancer. Nat
Genet 1997; 15:307-10. 16)
Dorozynski
A. Chaos. Br Med J 1989;298:350-1. 17)
Goldberger AL, Lipsitz LA. Andamenti frattalici e rigidità patologiche.
Sfera. Editrice Sigma Tau, n 36:62-5. 18)
Stagnaro-Neri M, Stagnaro S. Aritmia splenica, segno attendibile di
patologia bilio-duodenale. Minerva Med, 1985;76:30-1 [Pub-Med
indexed for Medline]. 19) Stagnaro-Neri M. Stagnaro S. Ketanserina, antagonista dei recettori 5 HTi serotoninergici e scavenger dei radicali liberi epatici. Clin Ter l992;l4l:465-73 [Pub-Med indexed for Medline]. 20) Stagnaro-Neri
M, Stagnaro S. Valutazione percusso-ascoltatoria del sistema nervoso
vegetative e del sistema renina angiotensina, circolante e tessutale. Arch Med Int 1992;3:173-92. 21) Stagnaro-Neri M, Stagnaro S. Aritmia splenica, segno attendibile di
patologia bilio-duodenale. Minerva Med, 1985;76:30-1 [Pub-Med
indexed for Medline]. 22) Stagnaro-Neri M, Stagnaro S. Vasomotility e Vasomotion nelle flebopatie ipotoniche istangiopatiche: caos deterministico e unita microvascolotessutale. Comun.Congresso Naz Soc It Flebologia Clin e Speriment, Catania, 4-7/12/1993. 23)
Firth WJ. Chaos—predicting the unpredictable.
Br Med J 1991;303:1565-8. 24)
Glenny RW, Robertson AT. Fractal properties of pulmonary blood flow:
characterization of spatial heterogeneity. Am Physiol Soc 1990:531-45. 25)
Freeman WJ. Strange attractors that govern mammalian brain dynamics shown
by trajectories of electroencephalographic (EEG) potential. Transaction on
circuits and systems. Brain, 1988;35:781-4. 26) Stagnaro-Neri M, Stagnaro S. Sindrome di Reaven, classica e
variante, in evoluzione diabetica. II ruolo della carnitina nella
prevenzione primaria del diabete mellito. II Cuore 1993;6:6l7-24. [Pub-Med
indexed for Medline]. 27) Intaglietta M,
Allegra C. Vasomotion and flowmotion. Minerva Angiol 1992;17 (Suppl 2 al N
2):215-8. 28) Intaglietta M, Breit GA. Vasomotor activity. In: Progress in applied
microcirculation. Basel:
Karger, 1988:25-32. 29)
Intaglietta M, Allegra C. Vasomotion and flowmotion. Minerva Angiol
1992;17 (Suppl 2 al N 2):215-8. 30) Curri SB. Rapporti
tra vasomotilita, periangio, sostanza fondamentale del connettivo e
linfatici. Minerva Angiol 1992;17(Suppl 2 al N 2):181-9. 31)
Folkow B. Description of the myogenic hypothesis. Circulat Res 1964;l4-15(Suppl):1279-85. 32) Peitgen HO, Richter
PH. La bellezza dei frattali. Immagini di sistemi dinamici complessi.
Torino: Ed Bollati Boringhieri, 1991. 33)
Ruelle D. Caso e caos. Torino: Ed Bollati Boringhieri, 1992. 34) Stagnaro-Neri M, Stagnaro S. Cancro della mammella: prevenzione
primaria e diagnosi clinica precoce con la percussione ascoltata. Gazz
Med It - Arch Sci Med 1993;
11-.447-57. 35) Peters MA., Stanford JL., Badzioch MD., et al. Genome-wide
scan for high-risk prostate cancer families with breast cancer reveals new
loci for prostate cancer and breast cancer. Nature
Genetics
36)
Stagnaro S., Istangiopatia Congenita Acidosica Enzimo-Metabolica
condizione necessaria non sufficiente della oncogenesi. XI Congr. Naz.
Soc. It. di Microangiologia e Microcircolaz. Abstracts, pg 38, 28
Settembre-1 Ottobre, 1983, Bellagio. 37) Stagnaro S., Istangiopatia Congenita Acidosica Enzimo-Metabolica. X Congr. Naz. Soc. It. di Microangiologia e Microcircolazione. Atti, 61. 6-7 Novembre, 1981, Siena. 38)
Stagnaro S., Istangiopatia
Congenita Acidosica Enzimo-Metabolica. Una Patologia Mitocondriale
Ignorata. Gazz
Med. It. – Arch. Sci. Med. 144, 423, 1985 (Infotrieve). Last update: 17 October 2002 |