|
These pages will hold papers which aim to illustrate both sense and significance (Den Sinn und die Bedeutung) of the new physical semeiotics, i.e., Biophysical Semeiotics, and personal view-points on Medicine Kingdom. Today,
at the begin of third millenium, one feels mostly the necessity of
efficacious physical semeiotics, which rather than substitute the older,
academic, traditional one, complete it, enlarging its border. The
descovery of numerous constitutions and Pre-Metabolic Syndrome makes
possible the real and successful primary prevention of the most common
and serious human diseases. In fact, the
possibility to recognize, e.g., both Oncological Terrain and
Oncological Real Risk allows doctor to perform malignancy primary
prevention, which is different from the screening realized now-a-days
all over the world. The open letter to Mr Ministro della Salute Prof.
Sirchia, regarding a biophysical-semeiotic model of breast cancer
primary prevention on very large scale outlines clearly the already
reached achievements, in the interest of diseased men, physician’s
profession dignity, and finally NHS budget. |
|
|
|
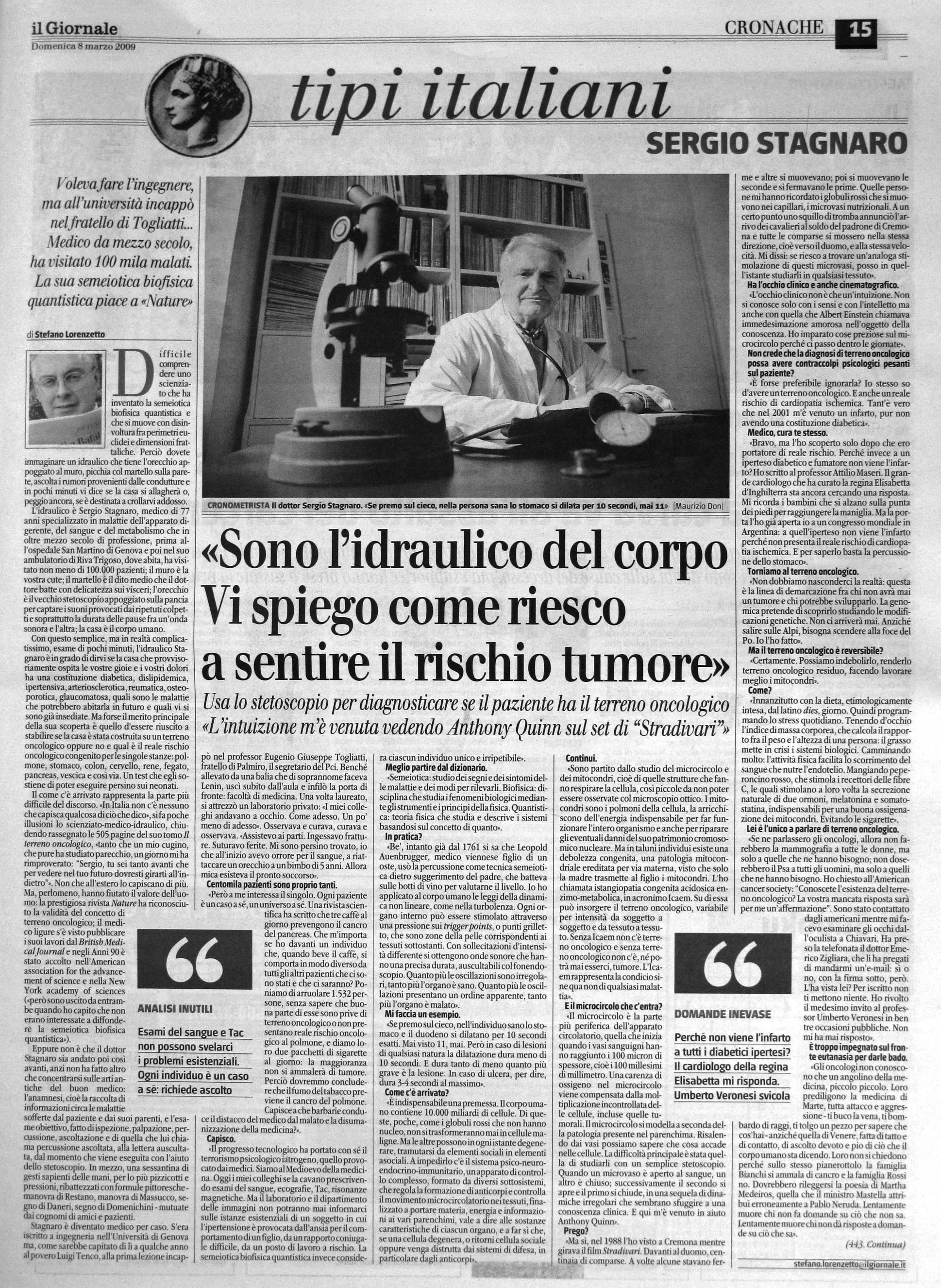
08.03.2009 - Article on a National Italian Newspaper
|
|
|
|
02.12.2008 - Links. http://wordpress.com/tag/dr-sergio-stagnaro/ http://www.mednat.org/curriculum_stagnaro.htm |
|
|
|
20.09.2008 - Importance of Knowing Quantum Biophysical Semeiotics. Notoriously, from the epistemiological viewpoint, a physical-semeiotic theory for being accepted from world-wide medical class must necessarily be more valid, giving a larger number of information than the previous one, that, among others considerations, has exceeded many controls in the course of the time (1-10). In following, some among the main reasons that justify the necessity and the usefullness of the acquaintance of Quantum Biophysical Semeiotics by doctors, are illustrated (11-21). 1) Quantum Biophysical Semeiotics allows doctors to bedside recognize in one second Oncological Terrain, even “latent” or “residual” (1), otherwise difficult to be diagnosed, conditio sine qua non of the malignant tumors, both solid and liquid. The acquaintance of this predisposition to malignancy, genetically directed and transmitted generally by the mother, renders the selection of the subjects with oncological terrain possible and, moreover, it facilitates bedside recognizing the real location of their risk, estimated in a “quantitative” way, base of cancer primary prevention, in "all" individuals predisposed to this pathology. Fortunately, the individuals can nowadais be selected and enlisted in a rational way, avoiding useless and expensive examinations in about 65 % of all cases, always conduct partially and not adequately, ending in enormous expenses for the SSN, and causing serious and avoidable worries for those who are free from oncological terrain, and obtaining very poor results (2). 2) Quantum Biophysical Semeiotics allows the rapid diagnose of numerous constitutions, even “latent”, among which the dyslipidaemic "and" diabetic constitution, conditio sine quan non of the type 2 diabetes (that is about 95% of all the cases). An efficacious primary prevention of the type 2 diabetes in individuals at inherited real risk, is today clinical and is founded on the diet, etimologically speaking, and on the histangioprotective drug use, as Melatonine (3, 4, 5, 10). 3) Quantum Biophysical Semeiotics permitts to recognize in a few seconds the Pre-Metabolic Syndrome, classic and variant, the later conditio sine quan non not of lithiasis (1). It follows to the several constitutions with the related inherited “real risk” (diabetic, dyslipidaemica, hypertensive, gouthy, osteoporotic, etc.) and can precedes of years or decades the Metabolic Syndrome, that can end in notes metabolic and cardiovascular pathologies, actual epidemics (1, 3, 5, 6) (V. http://www.semeioticabiofisica.it Practical Applications, 6 articles on Mellito Diabetes). The Pre-Metabolica Syndrome represents the "locus" of the Primary Prevention appliable on very large scale in individuals rationally selected. 4) Quantum Biophysical Semeiotics allows clinicians to recognize rapidly and quantitatively tissue level ofimportant citochine of the adipose tissue, like Adiponectine and the Leptin, which, through the stimulation of PPARs, play a primary role in the glico-lipidic metabolism and aterogenesis (http://www.semeioticabiofisica.it, Practical Applications). In addition, doctor can monitor at the bed-side the metabolic-endocrine state in objective way, express and reproducable according to need (Bibliography in the site). 5) Quantum Biophysical Semeiotics permitts early and rapid diagnosis of numerous and common human diseases (including appendicitis) (1, 9) facilitating the diagnostic iter and reducing the HNS expense (e.g., avoiding useless hospitalization and the excessive recource to the laboratory and the department of the images). 6) Quantum Biophysical Semeiotics allows doctor to exclude in one second whatever disorder, both possible or overt, independently of its nature. This aspect plays a central role in the importance of knowing the new physical semeiotics. In fact, the absence of gastric aspecific reflex, simultaneous to “intense” stimulation, for instance, of a thyroid trigger-point, allows to exclude present and future disorder of thyroid, benign or malignant in nature. Analogously, the absence of CAD inherited real risk indicates that these coronary vessels will not involved by such as disorder, even in presence of well-known, 300 environmental risk factors! (22-24). This is an epochal event, whose role is paramount in bot diagnosis and primary prevention. As a matter of fact, such as manoeuvre facilitate enormously diagnostic iter in a revolutionari way. 7) Quantum Biophysical Semeiotics allows to make “clinical” tele-diagnosis, utilizing both doctor and patient only a phone to cumunicate. As a consequence, it represents an epochal change in the care for humans involved by disorders, e.g., in the sea and mountains.
In conclusion, doctors have to realize that there are two different Medicine, the old, acadèmic, traditional one, and the “new”, really 50 year-old one, based on the fact that in all biological systems, including the microcirculatory bed, where deterministic chaos plays a pivotal role, besides local realm there is also no local realm (11-21). Formerly, with the aid of Biophysical Semeiotics, originated by the old auscultatory percussion, I described the microcirculatory bed as deterministic chaotic byological system, especially under physiological conditions In fact, in a lot of papers, I underlined both the biological significance of microvascular deterministic chaos, vasomotility and vasomotion, of all tissues and organs, and the central role in diagnosing, according to Angiobiopathy Theory(1-8) (See http://www.semeioticabiofisica.it). In health, we observe at the bed-side by means of a large number of reflexes, untill now unknown, unpredictable, irregular microvessel oscillations in all tissues. Interestingly, since November 2007, I have applied Quantum Biophysical Semeiotics in the study of biological systems (11-21). On the contrary, slow or rapid appearing of regular, and predictable microvessel fluctuations shows a typical pathological disorder, chronic and respectively acute. In a 52-year-long clinical experience this original evaluation proved to be a usefull and reliable tool in bed-side diagnosis, prevention, therapeutic monitoring and research. References. 1. Stagnaro Sergio, Stagnaro-Neri Marina. Introduzione alla Semeiotica Biofisica. Il Terreno oncologico”. Travel Factory SRL., Roma, 2004. http://www.travelfactory.it/semeiotica_biofisica.htm 2. Stagnaro S., Stagnaro-Neri M., La Melatonina nella Terapia del Terreno Oncologico e del “Reale Rischio” Oncologico. Ediz. Travel Factory, Roma, 2004 3. Stagnaro S., Stagnaro-Neri M., Le Costituzioni Semeiotico-Biofisiche.Strumento clinico fondamentale per la prevenzione primaria e la definizione della Single Patient Based Medicine. Ediz. Travel Factory, Roma, 2004. http://www.travelfactory.it/semeiotica_biofisica.htm 4. Stagnaro S., Stagnaro-Neri M., Single Patient Based Medicine.La Medicina Basata sul Singolo Paziente: Nuove Indicazioni della Melatonina. Travel Factory SRL., Roma, 2004. http://www.travelfactory.it/semeiotica_biofisica.htm 5. Stagnaro S. Pivotal role of Biophysical Semeiotic Constitutions in Primary Prevention. Cardiovascular Diabetology.2003, 2:1, http://www.cardiab.com/content/2/1/13/comments#5753 6. Sergio Stagnaro Biophysical Semeiotic Constitutions, Genomics, and Cardio-Vascular Diseases. BMC Cardiovascular Disorders 2004, http://www.biomedcentral.com/1471-2261/4/20/comments#95454 7. Stagnaro Sergio. Bed-Side Evaluating Breast Cancer Real Risk. World Journal of Surgical Oncology. 2005, 3:67doi:10.1186/1477-7819-3-67. 8. Stagnaro Sergio. Bedside Assessing ANS, RAAS, and IIR: a complex Relation to type 2 Diabetes. Cardiovascular Diabetology,15 November 2005. http://www.cardiab.com/content/4/1/15/comments#215501 9. Stagnaro-Neri M., Stagnaro S., Appendicite. Min. Med. 87, 183 [Medline] 10. Stagnaro Sergio Biophysical-Semeiotic Bed-Side Evaluating PPARs Activity in Metabolic Syndrome. Cardiovascular Diabetology. (19 September 2005) http://www.cardiab.com/content/4/1/14/comments#211488 11. Stagnaro Sergio e Paolo Manzelli. L’Esperimento di Lory. Scienza e Conoscenza, N° 23, 13 Marzo 2008. http://www.scienzaeconoscenza.it//articolo.php?id=17775 12. Stagnaro Sergio. Reale Rischio Congenito di Cancro Renale Diagnosticato con la Semeiotica Biofisica: il Segno di Pollio. www.ilpungolo.com, 25 Marzo 2008, http://www.ilpungolo.com/leggi-tutto.asp?NWS=NWS5480&IDS=13 13. Stagnaro Sergio. Il Cammino della Medicina : Semeiotica Biofisica Quantistica.Mutazioni Genetiche E Disfunzioni Dei Sistemi Biologici. www.ilpungolo.com, 30 Aprile 2008, http://www.ilpungolo.com/leggi-tutto.asp?NWS=NWS5548&IDS=13 14. Stagnaro Sergio. Melanoma? Escluso in 1 Secondo con La Semeiotica Biofisica Quantistica. Il Reale Rischio Congenito di Melanoma. www.ilpungolo.com, 9 Aprile 2008, http://www.ilpungolo.com/leggi-tutto.asp?IDS=13&NWS=NWS5524 15. Stagnaro Sergio. Diagnosi clinica di cuore sano in un secondo! 7 Aprile 2008. www.fce.it http://www.fcenews.it/index.php?option=com_content&task=view&id=1218&Itemid=47 16. Stagnaro Sergio. Non Local Realm. Response to Selection for Social Signalling Drives the Evolution of Chameleon Colour Change. (01 February 2008). www.plos.com, http://biology.plosjournals.org/perlserv/?request=read-response&doi=10.1371/journal.pbio.0060025 17. Stagnaro Sergio. Semeiotica Biofisica Quantistica: Diagnosi Precoce e Rapida di Metastasi Ossee 15 Gennaio 2008. http://www.ilpungolo.com/leggi-tutto.asp?IDS=13&NWS=NWS5308 2008 18. Stagnaro Sergio. La Diagnosi Clinica nella Semeiotica Biofisica Quantistica. www.fce.it 02-05-2008, http://www.fcenews.it/index.php?option=com_content&task=view&id=1285&Itemid=47 2008 19. Stagnaro Sergio. Role of NON-LOCAL Realm in Primary Prevention with Quantum Biophysical Semeiotics. www.nature.com, 01 Feb, 2008-05-17 http://www.nature.com/news/2008/080130/full/451511a.html 2008 20. Stagnaro Sergio. Bedside recognizing Inherited CAD Real Risk. www.natura.com 21 May, 2008. http://network.nature.com/forums/pmgs/1587?page=1#reply-4262 2008 21. Stagnaro Sergio. Bed-Side Biophysical-Semeiotic Evaluation of Thyroid Dysfunction in Cardiology. Ann Int Medic. 21 May, 2008, http://www.annals.org/cgi/eletters/0000605-200806030-00225v1 2008 22. Stagnaro Sergio e Manzelli Paolo. Semeiotica Biofisica Quantistica: Livello di Energia libera tessutale e Realtà non locale nei Sistemi biologici. www.fce.it , 29 maggio 2008, http://www.fcenews.it/index.php?option=com_content&task=view&id=1421&Itemid=47 23. Stagnaro Sergio. Role of Coronary Endoarterial Blocking Devices in Myocardial Preconditioning - c007i. Lecture, V Virtual International Congress of Cardiology. 2007. http://www.fac.org.ar/qcvc/llave/c007i/stagnaros.php 24. Stagnaro Sergio. Overlooking CAD Inherited Real Risk CAD Occurrence Will Continue! Medical News Today, 2008. http://www.medicalnewstoday.com/youropinions.php?opinionid=32629 25. Stagnaro Sergio. Bedside evaluation of cad biophysical-semeiotic inherited real risk under nir-led treatment. www.melatonina.it, 2008. http://www.melatonina.it/articoli/55-2008-09-01.html |
|
|
|
28.05.2006 -Biophysical-Semeiotic
Criteria of Diagnosing Metabolic Syndrome: Difference between
Pre-Metabolic and Metabolic Syndrome
Because
of 50-years in clinical experience, I partially agree with the
authors’ conclusions in the joint statement from the American Diabetes
Association and the European Association for the Study of Diabetes (1).
They rightly underscore "that too much critically important
information is missing to warrant its designation as a syndrome".
In fact, nowadays clinicians "should evaluate and treat all CVD
risk factors without regard to whether a patient meets the criteria for
diagnosis of the "metabolic syndrome" (1). The
fact is there are a growing number of physicians who are capable of
early recognition of Pre-Metabolic Syndrome and after years or decades,
identify the metabolic one, which always follows the former (2, 3). In
addition, at the base alteration in these syndromes there are both
parenchymal and microvascular inherited alterations, which parallel the
former, according to my theory of Angiobiopathy, which completes
Tischendorf's Angiobiotopy theory (2-6).
In
order to clinically define a particular constitution and related real
risk, which does not exclude the presence of several constitutions, it
is necessary to consider a present possibility of gathering
biophysical-semeiotic data at the bedside. This would include the necessary biological and
molecular-biological information on the various human organs, tissues
and biological systems, and at the same time reveal numerous types of
biophysical-semeiotic constitutions (even from the quantitative point of
view). Without
any doubt, these data cannot be observed in either traditional physical
or sophisticated semeiotics. On
a larger scale, the latter, is unable to carry molecular-biological
events to clinical dimension, which represents the most original and
fertile aspect of Biophysical Semeiotics and allows the doctor to
correctly diagnose Pre-Metabolic and Metabolic Syndrome. In addition,
despite the level of physical examination performed, sophisticated
semeiotics are expensive, making their use on a large scale basis
unlikely. I am sure that going beyond the traditional risk factors
represents a new medical "Weltanschauung".
In addition it would require open-minded physicians as "peer-reviewers",
though unfortunately seem harder to find in present times. References.
|
|
|
|
24.03.2006 - Oncogenesis is Oncological Terrain-dependent. Molecular
Lab: http://www.molecularlab.it/news/commento.asp?n=3823&comid=4255 Firstly I precise that for many years have been member of the AAAS (for health reasons!!! Now I’not); secondly I admit that PLOs.com kindly has posted recently a my wide comment (Stagnaro Sergio. Single Patient Based Medicines: its paramount role in Future Medicines. Public Library of Science, 2005, http://medicine.plosjournals.org); finally that from at least ten years my biography is published every year (even in 2007 Edition) on Who' s Who in America... and other volumes of the sort published in the States, including most famous one of the North Carolina... I state all that in order to avoid misinterpretions. O Moreover, I assert that every researcher would have to study PHILOSOPHY well, in this case Hume. Conditio sine qua non of the oncogenesis is represented by a congenital alteration – transmitted from mother like all other mitochondrial citopathy - of the psico-neuro-endocrine-of immunity system, that it is based exactly on a singular mitochondrial pathology. In this predisposition, as the title descriptive indicates clearly, a primary role is carried out from the reduced immune system. I would want to say american friends that presence of bacteria (innocent bystander) in the center of a tumor, either mammary or pancreatic or tyroid, or prostatic a.s.o....., as the following "simplest" clinical evidence demonstrates: the tumor ALWAYS is present in subject Oncological Terrain- positive, BUT in the precise location – recognized since BIRTH - of the oncological "Real Risk" detected with the aid of Biophysical Semeiotics (See in this website Oncological Terrain, and Bibliography). In other words, individuals positive for Oncological Terrain, BUT without oncological "Real Risk" in the prostate will not never suffer from prostatic cancer, regardless the type of life style, as 50-year-long clinical "experience allows me to state " (sic!). |
|
|
|
27.12.2005 - Letter to Minister Storace about Oncogenesis Dear
Minister of the Health, On. Francesco
Storace, Rome. Today
is Christmas and I am sure that you, too, are thinking that I would have
do much better to put between parenthesis the problems that harass us
day after day and to enjoy the peace that this Holy Day gives to the men
He loves. However, the problems, I am speaking of, are really singular,
interesting not only who write, but also about 33% of the Italian
population, who are positive for Oncological Terrain.
Moreover, I, ahead in the years, remember with precision that the Lord
has admonished us to always watch, because we do not know when He will
call us to the house of the Father. The unfortunate outcome of two my
previous Open Letters, sended to the former Ministers of the Health,
makes me forsee that also this claim of mine will reveal a "vox
clamantis in desert". A result of primary importance has already
been caught up however: my conscience is clean like always. I
would like, Mr. Minister of the Health, to tell you of a new way of war
against cancer, realizable without any expenses for the NHS on very
large scale, i.e., on entire population involved by Oncological Terain,
and, most important, by "Real Risk" of tumour. At this point,
On. Francesco Storace, since You completely ignore these concepts of
Clinical Oncology, You will surely ask yourself what I’m speaking of. No
worry! These terms, in fact, are overlooked completely also by italian
oncologists and "ignored" by the two former Ministers,
mentioned above. I am truly happy, instead, because in foreign countries
the results of my clinical researches, gathered with the aid of
Biophysical Semeiotics, are taken into critical consideration and
published. For instance, Mr. Minister you can read my comment recently
posted by an world-known
USA website: <<<
Mutations in
the mitochondrial DNA D-loop region are frequent in cervical cancer Comments
on this article
(1) Mitochondrial Bed-Side Evaluation: a new Way in the War
against Cancer. http://www.cancerci.com/content/5/1/34/comments
Mitochondrial
Bed-Side Evaluation: a new Way in the War against Cancer. Sergio
Stagnaro (21 December 2005) Biophysical
Semeiotics Research Laboratory. I
agree with the autors’s conclusions of this interesting paper (Himani
Sharma, Archna Singh, et al. Mutations in the mitochondrial DNA D-loop
region are frequent in cervical cancer Cancer Cell International 2005,
5:34 doi:10.1186/1475-2867-5-34). In fact, in previous articles, I
referred that, as a working hypothesis, I thought a long time ago that
all chromosomal alterations, of whatever nature, both n-DNA and m-DNA,
are necessarily accompanied with similar microvascular modification of
the local microcirculatory bed, both structural and functional in
nature, in subjects involved by abnormalities of
pschyco-neuro-endocrinological-immune system, i.e., in malignancy
biological control system, I defined as Oncological Terrain (1-6).
Really, both genetical and environmental factors induce
contemporaneously parenchymal and microvascular cell alterations,
according to the well-known concept of Tiscendorf’s Angiobiotopie, I
completed with Angiobiopathy new concept (1). In a few words, all
oncological cell-dependent events (control, regulation, duplication,
a.s.o.), may happen only by means of singular changes in local
structural and functional microcirculation, which notoriously supplies
information-material-energy to related tissue cells (See my web sites http://www.semeioticabiofisica.it
and Now-a-days,
thanks to Biophysical Semeiotics, we can fortunately evaluate clinically
microcirculatory bed structure and function in a precise manner, e.g.,
of breast cancer real risk, and cancer, of course, of all other
biological systems, including lymphnodes and bone-marrow, assessing
clinically local vasomotility and vasomotion (1-6). Evaluating properly
the type of microcirculatory activation of cancer as well as of local
lymphnodes and bone-marrow (type I, associated, physiological; type II,
intermediate, partially dissociated, characteristic of real oncological
risk, and finally type III, dissociated, indicating cancer onset) we can
evaluate in a quantitative way the alterations of physiological relation
between vasomotility (= chaotic deterministic oscillations of small
arterioles and arterioles, according to Hammersen, on the one hand, and
vasomotion (= chaotic deterministic oscillations of related capillary
and post-capillary primary venules), since the intensity of such as
dissociation is correlated with the seriousness of underlying
oncological disorders. 1)
Stagnaro Sergio, Stagnaro-Neri Marina. Introduzione alla Semeiotica
Biofisica. Il Terreno oncologic. Travel
Factory SRL., Roma, 2004. 2)
Stagnaro S., Stagnaro-Neri M., Le Costituzioni Semeiotico-Biofisiche.Strumento
clinico fondamentale per la prevenzione primaria e la definizione della
Single Patient Based Medicine. Ediz.
Travel Factory, Roma, 2004.
http://www.travelfactory.it/semeiotica_biofisica.htm 3)
Stagnaro-Neri M., Moscatelli G. Stagnaro S., Biophysical Semeiotics:
deterministic Chaos and biological Systems. Gazz. Med. It. Arch. Sc. Med.
155, 125 ,1996 4)
Stagnaro Sergio. "Genes, Oncological Terrain, and Breast Cancer"
World Journal of Surgical Oncology., 2005, http://www.wjso.com/content/3/1/45/comments#205475 5)
Stagnaro Sergio. Relevance of Mitochondria in Cancerogenesis. Journal
of Carcinogenesis. 2005, 4:1 doi:10.1186/1477-3163-4-1http://www.carcinogenesis.com/content/4/1/1/comments#136454 6)
Stagnaro Sergio. Bed-Side Evaluating Breast Cancer Real Risk. World
Journal of Surgical Oncology. 2005, 3:67 doi:10.1186/1477-7819-3-67.
2005>>>. I am perfectly aware of
the difficulties that involve changing paradigms in Medicine, to modify
the "Status Quo" in the field of Oncology, suggesting
physicians to follow new ways in the war against cancer: physicians who
are on old positions which proved to be insufficient, harmful,
insufficiently effective, based on bias, to often founded on wrong bases,
e.g., considering in the pathogenesis of cancer only the mutations of
the nuclear DNA, easier to study, overlooking the mitochondrial DNA (V. http://www.semeioticabiofisica.it,
Oncological Terrain, and Bibliography). My clinical experience of 49
years, formerly with the aid of Auscultatory Percussion, and then with
Biophysical Semeiotics, allows me to state that if the new concepts –
Oncological Terrain and oncological "Real Risk" are not
learned as well as utilised, we
will never be authorized neither to speak of, nor able of leading a
truly effective and not expensive war against cancer in individuals
rationally selected since birth. In such as original war against
malignancy, wherein General Practitioners will play a paramount role,
the diet, etymologically speaking, and the use of Coniugated-Melatonine,
according to Di Bella-Ferrari, represent the unavoidable tools to
utilize in personalized way. I hope, finally, that
this my open letter will fortunately find a favourable acceptance,
offering also to You the promise of my advise, based on a long firm
experience, but not surely my practical participation for health reasons.
Best regards Sergio
Stagnaro MD. General
Practitione. Retired Founder
of Biophysical semeiotics 16037
Riva Trigoso (Genova) Holy
Christmas 2005 |
|
|
|
10.09.2005
- Biophysical Semeiotics on indian prime medical website http://www.indmedica.it |
|
|
|
26.06.2005 - Necessity and usefullness of the acquaintance of the Symptomatology Biophysics. 1)
Biophysical Semeiotics has allowed the discovery of the
Oncological Terrain (1), conditio sine qua non of the malignant
tumors. The acquaintance of this predisposition to malignancy,
genetically directed and transmitted generally by means of the mother,
renders the selection of the subjects with oncological terrain possible
and, moreover, it allows quantitatively to recognize the real center of
their risk, estimated in a “quantitative” way, base of cancer
primary prevention, in "all" individuals predisposed to this
pathology. Finally, the individuals can properly be selected and
enlisted in a rational way, avoiding useless and expensive examinations,
always conduct partially and not adequately, ending in enormous expenses
for the SSN, and causing serious and avoidable worries for those who are
free from oncological terrain, and obtaining very poor results (2). 2)
Biophysical Semeiotics has allowed the description of numerous
constitutions, among which the dyslipidaemic "and" diabetic
constitution, conditio sine quan non of the type 2 diabetes (that
is the 90-95% of all the cases). The primary prevention of the type 2
diabetes is today clinical and is founded on the diet, etimologically
speaking, and on the histangioprotective drug use (3, 4, 5). 3)
Biophysical Semeiotics permitted to discover the Pre-Metabolic
Syndrome, classic and varied, the later conditio sine quan non
not of lithiasis (1), that follows
to the several constitutions (diabetic, dyslipidaemica, hypertensive,
gouthy, osteoporotic, etc.) and it precedes of years or decades the
Metabolic Syndrome, that can end in notes metabolic and cardiovascular
pathologies, actual epidemics (1, 3, 5, 6) (V.
www.semeioticabiofisica.it Practical Applications, 6 articles on Mellito
Diabetes). The Pre-Metabolica Syndrome represents the "locus"
of the Primary Prevention appliable on very large scale in individuals
rationally selected. 4) Biophysical Semeiotics allowed the description of methods reliable to clinicians, rapid on application and, therefore, usefull to doctor in bed-side assessing quantitatively important citochine of the adipose tissue, like Adiponectine and the Leptin, which, through the stimulation of the PPARs, play a primary role in the glico-lipidic metabolism and aterogenesis (www.semeioticabiofisica.it, Practical Applications). In addition, doctor can monitor at the bed-side the metabolic-endocrine state in objective way, express and reproducable according to need (Bibliography in the situated one). 5) Biophysical Semeiotics permitts early diagnosis of numerous and common humen diseases (including appendicitis) (7, 8, 9) facilitating the diagnostic iter and reducing the HNS expense (e.g., avoiding useless hospitalization and the excessive recource to the laboratory and the department of the images) References.
|
|
|
|
03.03.2005
- Is the Silence of
“all” National Health Service Authorities on Biophysical Semeiotics
ethical? The
following Rapid Response has been posted the 25 February, 2005 on the
website www.bmj.com and on the italian
website www.katamed.it Sirs, I
agree, of course, with the statement that “Ethical considerations
should apply to all medical practice, but many people act as
if they apply only to research”. However, I cannot define ethical the
behaviour of “all”
National Health Service Authorities, particularly the italian NHS
Authorithy, ethics
committees, journal editors, including BMJ, although posts kindly
my weekly Rapid Responses, a.s.o. (with
the only exclusion of “Planning
for the EU public Health Portal” at URL: References. 1)
Wade D.T.Ethics,
audit, and research: all shades of grey. BMJ 2005;330:468-471 (26 February),
doi:10.1136/bmj.330.7489.468 2) Stagnaro Sergio, Stagnaro-Neri Marina. Introduzione alla Semeiotica Biofisica. Il Terreno oncologico”. Travel Factory SRL., Roma, 2004. http://www.travelfactory.it/semeiotica_biofisica.htm 3)
Stagnaro S., Stagnaro-Neri M., Le Costituzioni
Semeiotico-Biofisiche.Strumento clinico fondamentale per la
prevenzione primaria e la definizione della Single Patient Based
Medicine. Ediz.
Travel Factory, Roma, 2004. 4) Stagnaro-Neri M., Stagnaro S., Cancro della mammella: prevenzione primaria e diagnosi precoce con la percussione ascoltata. Gazz. Med. It. – Arch. Sc. Med. 152, 447,1993 5)
Stagnaro-Neri M., Stagnaro S., Diagnosi Clinica Precoce
dell’Osteoporosi con la Percussione
Ascoltata. Clin.Ter.
137, 21-27, 1991 6)
Stagnaro S., Diet and Risk of Type 2 Diabetes.
N Engl J Med. 2002 Jan 24;346(4):297-298. letter [MEDLINE] |
|
|
|
09.02.2005
- Information-disinformation: who informs the informers! From
many years by now we have convinced themselves that the total
communication cancels the borders surely, and is this a positive side,
but at the same time he is not always in a position to supplying quality
and "democracy". We think, as an example, to the energetic
sources alternatives to the oil, possible, little expensive and
especially not polluting. Or we think next to the effective fight
against most common, serious, mortal or invalidating human diseases,
that they could be vanquished, in great part naturally, if the existence
of the several constitutions - diabetic, dislipidemica, hypertensive,
glaucomatous, arteriosclerotic, osteoporotic, lithiasic, and above all
oncological - if the so-called competent HNS Authorities as well as
Health Minister "honestly" would discusse about
“biophysical-semeiotc constitutions” and finally they will gives
these knowledges to the doctors, including those unwilling to medical
continue education, and to common people. In fact, beside the EBM also
SPBM does really exist (1-4 exists also). This favorable event is
unavoidable in order to rationally select in a precise way the
individuals that need really of primary prevention and the successive
therapeutic monitoring: the true progress of the humanity, after all,
often consists in removing the patina of the time to things already
known but forgotten. It must ask to us, as an example that sense has to
undertake a primary prevention against a defined pathology in
individuals that will not never suffer from this disease because you
deprive of the relative "constitution semeiotico-biophysics". References. 1) Stagnaro
Sergio, Stagnaro-Neri Marina. Introduzione alla Semeiotica Biofisica. Il
Terreno oncologico”. Travel Factory SRL., Roma,
2004. http://www.travelfactory.it/semeiotica_biofisica.htm 2)
Stagnaro
Sergio, Stagnaro-Neri Marina. La Melatonina nella Terapia del
Terreno Oncologico e del “Reale Rischio” Oncologico. Ediz. Travel Factory, Roma, 2004. 3) Stagnaro
Sergio, Stagnaro-Neri Marina. Le Costituzioni Semeiotico-Biofisiche.Strumento clinico fondamentale per la
prevenzione primaria e la definizione della Single Patient Based
Medicine. Ediz.
Travel Factory, Roma, 2004. 4) Stagnaro
Sergio, Stagnaro-Neri Marina. Single
Patient Based Medicine. La
Medicina Basata sul Singolo Paziente: Nuove Indicazioni della Melatonina.
Travel Factory SRL., Roma, 2004. |
|
|
|
19.12.2004 - Unified
Pathogenetic Theory
Does it really exist? What are her consequences for future Medicine? Link |
|
|
|
18.11.2004
- Biophysical Semeiotics becomes art
The picture outlines in a really artistic way Biophysical Semeiotics fundamental achievement, i.e., the definition of diverse constitutions, doctor can easily and rapidly recognize and quantify at the bed side. The artist will show how these scientific descoveries, all temporary in nature, are mainly based on former greatest Physician work.
Semeiotica BioPhisica (cm 100 x 80): affresco & assecco su intonaco Paola Contili (Avigliano Umbro, Terni) |
|
|
|
Lettera aperta al Ministro della Salute, Prof. Sirchia, sulla prevenzione primaria “clinica” del cancro mammario. http://www.katamed.it/Notizia.asp?id=8094&lingua=IT&idcat=999; [Such
as letter can be read in following URLs http://xoomer.virgilio.it/piazzetta/professione/professione.htm
http://www.ilpungolo.com/site/leggi.asp?NWS=2390&IDS=10
http://bmj.bmjjournals.com/cgi/eletters?lookup=by_date&days=1#72216
(27
August 2004)] To
the italian Minister of the Health, Prof. Sirchia. As
you knows very well, the screening of the cancer does not coincide at
all with the primary prevention of the malignant tumor: all SSN, in
Italy and the world, have lead and lead, with remarkable expenses,
"limited, fail to fulfill" and partially effective screenings
for breast cancer, but never one true campaign of primary prevention on
the entire, both male and feminine population: actually, also the male
sex can be hit from breast cancer. In truth, for being able to realize
successfully a primary prevention of a tumor between the most diffuse,
which causes elevated mortality and suffering, the doctors and the
competent sanitary authorities, must know the oncological constitution,
i.e., the Oncologico Terrain, and the Oncological Real Risk (1, 2) (See
web-site, HONCode 233736, www.semeioticabiofisica.it:
Oncological Terrain), component of the Single Patient Based
Medicines, suggested also from the Competent Authorities in
"Planning for the EU Public Health Portal", web-site Europe
Health Alliance, at this URL
(page 36) I write, Mr. Minister, this opened letter on "clinical" primary prevention of breast cancer for two reasons principally: A) a 47
year-long clinical experience allows me to state that “clinical”
primary prevention of breast cancer must unavoidably be preceded from
rational selection of "all" individuals of both sexes,
involved by Oncological
Terrain "and" Oncological Real Risk in a mammary quadrant (or
more, of course), recognizable and easily quantificated with the
Biophysical Semeiotics. B)
from
always I agree perfectly with following thought: "It is difficult
to remove methods perfectly organized, from the long tradition,
supported from famous names also, based on an elegant, but wrong
doctrinaire equipment; strong from political, economic, organizational,
financial, pseudosocial view-point. We dare to face such as paramount
problem, more than in the conviction to succeed and to resolve, in order
not to feel in guilt towards ourselves".(Luigi Di Bella: "Cancer:
we are on the just way?". Editions Travel Factory Srl - Rome,
2001). The
performance of this original intervention
of primary prevention of breast cancer, surely other that expensive, but
effectively involving "all" citizens with oncological real
risk, need of the essential participation of General Practitioners, who
play a role of primary importance. The
various stages of this prevention can be, generally, established as
follows, awaiting obviously the
definitive contributions by authorities specialized in this type of
operations concerning public health and by the ethical committees;
regarding eventually expectable objection, i.e., the possible
discrimination of the positive citizens for the Oncologico Land, I,
former-bearer of oncological constitution, put the question:” What
does it meanto spend huge sums of money in searches on the genetic code
and the mutations of "the single" DNA nuclear, in the light of
such suspects discrimination? 1)
In a city, Province or Region, firstly must be recognized the
individuals with Oncological Terrain and with Real Mammary Oncological
Risk, quickly and easy quantified; secondly,
they have to be recorded in complete way on an appropriate
document, to use in the successive controls. These individuals,
completely learned by their physicians about the causes and of the ends
of the prevention, are enlisted in the primary prevention organized and
directed by the ASLs, in ways to establish properly. 2) All the
subjects selected therefore undergo to the preventive dietetic measures
,meaning the diet in etimological sense, and treatment, personally
administered (1, 2). Due
to personal physical conditions, and not only because of my age, surely
I can not allow me to participate actively to this prevention, to which
I can only assure all the my "theoretical" contribution and of
competence in the Biophysical Semeiotics. I
thank you, Mr. Minister of the Health, for the kind acceptance. Best
regards and greetings of All God. |
Last update: March 18, 2018