|
GENE
MUTATIONS, MICROCIRCULATORY ABNORMALITIES, ONCOLOGICAL TERRAIN, AND
ONCOGENESIS (FIRST PART). First
part - Second part - Third
Part (Download)
From
Gene Mutations to Breast Cancer.
Localized
Tissue-Microcirculatory Unit Abnormalities in individuals at
risk for cancer.
Biophysical-Semeiotic
morphological analysis of vasomotion in both physiology and pathology.
In
the war against cancers, we must possibly find a “clinical” tool
that helps “all” doctors in bed side recognizing, in apparently
healthy, genetical errors, causing hyperinsulinemia-insulinresistance,
melatonine as well as endogenous oppioids deficiency, metabolic
disorders, prevalence of stress axis, a.s.o., which, in turn, can
aggravate chromosomal aberrations as those observed in cancer cells. In
fact, our target can be reached hopefully if “all” doctors are able
to ascertain, or at least suspect, clinically in otherwise healthy
people gene mutations, oncogenesis is based on, possibly long time
before cancer on-set. As
a working hypothesis, I thought previously (at the end of 1970) that all
gene mutations, of whatever nature, are necessarily accompanied with
similar microvascular modification, both structural and functional,
of the local microcirculatory bed in subjects involved by
abnormalities of pschyco-neuro-endocrinel-immune system, i.e. by
oncological terrain (See: “Oncological Terrain” in my site, HONCode
ID, N. 233736, http://digilander.libero.it/semeioticabiofisica). As
a matter of fact, both genetical and environmental factors can induce contemporaneously
parenchymal and microvascular cell alterations, according to the
well-known concept of Tischedorf’s “Angiobiotopie”. For instance,
a family of molecules called cyclins was descovered. It is through
changes in the production of cyclins during the cell cycle that the
activities of the genes controlling it are themselves regulated. All
these events (control, regulation a.s.o.), however, can happen only by
means of changes in local microcirculation, i.e., in supplying
information-material-energy to cells, which need to repair their damaged
n-DNA. Now,
thanks to Biophysical Semeiotics (See the above cited-site), we can
fortunately evaluate clinically both structure and function of the
microcirculatory bed, in a precise manner and in all biological system
(2-5). Based
on 45-year-long "clinical" experience, I think that the
decline in cancer rates all over the world could be more intense if
scientists will consider and discuss the possibility that the "Oncological
Terrain", based on Congenital Acidosic Enzyme-Metabolic
Histangiopathy, a mitochondrial functional cytopatology, almost always
eredited by mother, really exists. In
other words, as regards oncogenesis, we must consider not only n-DNA
abnormalities, but also alterations of m-DNA. As
a matter of fact, e.g., not all smokers, on the one hand, are involved
by pulmonary cancer, as well as not all people with chronic hepatitis,
on the other hand, will die of hepatocarcinoma. Moreover, in some
families malignancies occur more frequently than in others. Actually,
as I described in the above-mentioned papers, there are other
irrefutable as well as unavoidable causes that accounts for the reason
of existence of the oncological “real” risk, i.e. oncological
terrain, and consequently, Congenital Acidosic Enzyme-Metabolic
Histangiopathy, i.e. m-DNA abnormalities. At
this point, the first question is the following: "What
does characterize oncological terrain from the "clinical" and
microcirculatory point of view?". In
fact, in order to perform efficacious cancer primary prevention
on very large scale, it is unavoidable that the modifications occurring
in the biological controll system could be easily, promptly, and
“quantitatively” ascertained and properly evaluated at the bed-side,
i.e., with the aid of a “clinical” method, by the use of a
sthetoscope, and certainly without application of sophysticated but
expensive semeiotics, that may not be applyed in all individuals, that
is, on largest scale, because only a few doctors can utilize them. If
it is possible to answer this first question, a second one immediately
follows: "The
oncological terrain which certanly can be worsened by the negative
intervention of environmental factors, is also in some way, at least
partially, reversible?". It
is urgent and necessary to know if the oncological terrain can be
reversed, i.e., if it can totally or, at least, greatly disappear, with
the aid of drugs and/or diet, ethymologically speaking, which exert a
favourable influence on the characteristic modifications of the
psycho-neuro-endocrine-immunological system, that
just represent the “oncological terrain”. My
answers to these questions are readable in my above-cited site (5). The
war against cancer will be fortunately won if all doctor are able to
recognize, with the aid of a stethoscope, individuals apparently healthy
but positive for “oncological terrain”, particularly intense in a
well defined tissue region, who have to undergo immediately to proper
diet, ethymologically speaking, and therapy with histangioprotective
drugs, in some cases. At
this point, however, it is unavoidable to investigate and possibly
clarify the relation between gene mutations, including m-DNA alterations,
microcirculatory abnormalities, oncological terrain, and oncogenesis
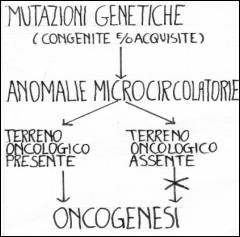
(Fig.1).
Fig. 1 Gene
mutations cause local
tissue-microvascular unit abnormalities,direcltly and/or indirectly,
e.g. AVA and DEB structural and functional alterations, blood-flow
centralization, tissue acidosis, a.s.o., which in turn, but exclusively
in presence of oncological terrain, based on Congenital Acidosis
Enzyme-Metabolic Histangiopathy, can bring about oncogenesis. From
Gene Mutations to Breast Cancer.
Cancer
results, notoriously, from the accumulation of mutations in genes
(n-DNA) that regulate cellular proliferation and these mutations can
occur early in the process of malignant transformation or later, during
progression to an invasive carcinoma. The inheritance of mutated allele
is commonly followed by the loss of the second allele from a somatic
cell, leading to the inactivation of a tumor-suppressor gene and
triggering malignant transformation. Genes
important to the development of cancer regulate diverse cellular
pathways, including the progression of cells through the cell cycle,
resistance to programmed cell death (apoptosis), and the response to
signals that direct cellular differentiation. Moreover, the inactivation
of genes that contribute to the stability of the genome itself can favor
the acquisition of errors in other genes that regulate proliferation.
The importance of this latter pathway in the development of breast
cancer is highlighted by two recent studies linking the function of the BRCAl
gene, implicated in the genetic predisposition to breast and ovarian
cancer, with that of the A1M gene, which in its mutant form
causes the genomic instability in ataxia-telangiectasia (6, 7) Errors
in n-DNA that arise during normal replication of the molecule (nucleotide
mismatches) or that are induced by ionizing radiation or genotoxic drugs
can cause mutations in coding sequences or breaks in double-stranded
chromosomal DNA. If the nucleotide mismatch is not repaired before a
round of DNA replication occurs, that mutation is transmitted to
daughter cells. A mitotic catastrophe can be caused by
an unrepaired break in double-stranded DNA when the cell attempts
to segregate broken chromosomes. Studies of yeast have identifìed genes
that sense damaged DNA and cause the arrest of the cell cycle, which
allows time for the molecular defect to be repaired. These genes operate
at several specific "checkpoints" in the cell cycle as a means
of ensuring genomic integrity before DNA is synthesized. The most
critical checkpoint gene yet identifìed that is related to cancer in
humans is the tumour-suppressor p53, not essential for cell viability,
but critical for monitoring damage to DNA. Inactivation
of p53 is an early step in the development of many kinds of tumors.
Patients with the Li-Fraumeni syndrome usually carry one mutant
germ-line p53 allele and are at risk for the development of
sarcomas, leukemia, and cancers of the breast, brain, and adrenal glands.
In rare cases of the Li-Fraumeni patients do not have a germ-line p53
mutation, but they may have a mutation in CHK2, a gene encoding a
protein kinase that directly activates p53 protein by adding a phosphate
group to it (7 8). The Li-Fraumeni syndrome is rare, but in over half of
all sporadic cases of cancer, p53 is inactivated at some point during
the progression of the disease. In cases of cancer without p53 mutations
there are frequently alterations in two other genes - MDM2 and pl4ARF
-that regulate the expresion of p53. The
sensing of breaks in DNA and the activation of p53 require ATM.
This gene encodes a kinase that activates both CHK2 and p53
in response to damaged DNA. Children
with ataxia-telangiectasia have inactivating mutations in both ATM
alleles and have immunodeficiency, cerebellar abnormalities, and a
predisposition to cancer, primarily lymphomas. Their cells fail to
activate p53 in response to damaged DNA, demonstrate genomic instability,
and are extremely sensitive to genotoxic agents. A similar disorder, the
Nijmegen breakage syndrome, is caused by homozygous inactivation of the NBS
gene. The NBS protein appears to be directly involved in the repair of
breaks in double-stranded DNA. The recent observation that NBS is
activated by ATM after DNA is damaged identifies a cellular pathway that
can account for the similar clinical consequences of mutations in these
two genes.(10, 11) Into
this pathway of response to damaged DNA enters the BRCAl gene.
Mutations in one germ-line allele of BRCAl are responsible,
according to some authors, but not to others, for approximately half of
all cases of familial breast cancer. The normal function of the BRCAl
protein remains elusive, but important information has emerged from the
identification of other proteins that interact with it. The discovery
that both ATM and CHK2 can add phosphate groups to the BRCAl protein
after n-DNA is damaged (6, 11) and that the phosphorylated BRCAl is
relocalized within the nucleus suggests that it, too, may participate in
the response to damaged n-DNA. ATM can also phosphorylate a BRCAl
cofactor, CtlP, that regulates gene transcription (7) and there are
indications that BRCAl protein is part of a complex that includes NBS
and other DNA-repair proteins (13). The current data suggest that BRCAl
is critical for the repair of double-stranded breaks in chromosomes.
These new insights raise important questions about the genetic events
that lead to breast cancer. Why should breast epithelial cells be more
susceptible than other types of cells to the consequences of the genomic
instability caused by loss of function of the BRCAl gene? And why should
breast cancer develop in carriers of a mutant germ-line BRCAl
allele after the somatic loss of the second BRCAl allele, whereas BRCAl
is rarely if ever inactivated in patients with sporadic breast cancers?
No answers to these questions have yet emerged, but the susceptibility
of breast tissue to DNA damage may reflect the repeated cycles of
estrogen-driven cellular proliferation that occur normally in this
tissue. As for why the inactivation of BRCAl occurs only in cases
of familial breast cancer, it is possible that inheritance of one mutant
BRCAl germ-line allele increases the likelihood that a breast
epithelial cell will lose the second allele before the occurrence of the
estrogen-driven proliferation associated with puberty. Mutations
in BRCAl and BRCA2 have been associated with an increase
in the lifetime risk of breast cancer by a factor of more than 20, but
these highly penetrant mutant alleles are relatively rare in the general
population. In contrast, 1% of the population carries an inactive ATM
allele. Some studies have suggested that such relatively common alleles
are associated with a moderate increase in the risk of breast cancer,
although the magnitude of this increase is debated (14, 15). Completion
of the human-genome project and other advances are likely to uncover
additional common variations within a host of novel genes implicated in
the response to n-DNA damage. Defining the possible adverse or even
protective contribution of these genetic variations to the development
of breast cancer and marshaling this information to improve clinical
care will be the challenge. In
addition, authors demonstrated recently that in carriers of BRCA1
mutations, the overall increased risk of cancer at sites
other than breast and ovary is small and is observed in women
but generally not in men. BRCA1 mutations may confer
increased risks of other abdominal cancers in women and
increased risks of pancreatic cancer in men and women (36). Localized
Tissue-Microcirculatory Unit Abnormalities in individuals at
risk for cancer. At
this point, continuing present discussion, analyzing breast cancer as
example, I will illustrate briefly localized tissue-microcirculatory
unit inherited abnormalities, i.e., in the precise site of risk
for malignancy and obviously in the area of cancer
itself, after discussing the biological significance of microcirculatory
deterministic chaos (For further information, see http://digilander.libero.it/microangiologia). Chaos,
a mathematical concept, has been described as "deterministic
randomness", meaning that a chaotic system is deterministic, but so
complicated that looks random. Chaos theory tells us it is impossible to
predict the long term behaviour of very complex systems, because all the
conditions are not known with precision at any time and uncertanty
increases with time (16) . It
is well known that electrocardiograms, for example, of healthy hearts
constantly vary, however slightly, in an unpredictable way. But in dying
patient the intervals between beats (R-R) become practically identical
and electrical signals predictably cyclic (17). We
described in previous papers, for the first time clinically, spleen
(18), liver (19), kidney (20) and pancreas (20) chaotic oscillations,
partly due to Autonomic Nervous System activity. More
precisely speaking, organ and tissue oscillations are related to their
local microvessels chaotic activity, i.e. the complexity of the dynamism
of the firsts corresponds exactly to that of the second. In addition,
the physiologically functioning organ presents complex, chaotic
oscillations, constrained to a “strange attractor” in the phase
space (See later on). On
the contrary, in a diseased organ there are cyclic, periodic, regular,
identical, predictable and low oscillations without highest spikes
(HS). In
conclusion, the microcirculatory bed and consequently the related
organ as biological dynamic system loses complexity, it loses its
adaptative capacity and ability to responde (16). Interestingly,
biophysical-semeiotic evaluation of the complexity degree is very
important as regards prevention, diagnosis and therapeutic monitoring. As
mentioned above, the chaotic size fluctuations of kidney, pancreas,
liver, spleen, aorta, heart (obviously, regardless systo-diastolic
movements), a.s.o. are due to their congestion and decongestion (6
cicles per minute) as clinical and experimental evidence suggests. In
facts, organs chaotic oscillations are strictly analogous and
synchronous with related microvessels fluctuations, presenting really
identical behaviour . Consequently,
we are allowed to state that chaotic behaviour of local nutritional
capillaries and venules brings about volume randome changing of the
related organs, mentioned above. Therefore, it is easy and reliable to
assess in a precise manner oscillations of about all organs and tissues
by means of the evaluation of corresponding microvessels fluctuations. In
other words, besides kidney, pancreas, heart, spleen, liver, a.s.o.,
chaotic oscillations assessment, it is practical, usefull and reliable
to evaluate the "oscillations" of important tissues, organs
and glands, such as bone-marrow, prostate, lungs, gall-bladder, breast,
urinary-bladder, stomach-duodenum, a.s.o. (18, 20, 21), evaluating vasomotility
and vasomotion of related microcirculatory bed. As
regards bone marrow and breast, for example, digital pressure upon the
middle line of breast-bone (and/or hyliac crests) and mammary gland,
respectively, in healthy, brings about choledocic "arteriolar",
"venular" reflexes as well as upper (=small arteries and
arterioles, according to Hammersen) and lower ureteral reflex (=
nutritional capillaries), which fluctuate in a chaotic manner, as
mentioned above. Interestingly, moreover, AP values of marrow- and
mamma-oxygenation and CoQlO levels (34) are in perfect relation with
fractal dimension of chaotic choledocic and ureteral fluctuations. At
this point, it appears relevant to outline that during acute disorder,
flogistic in nature, local periodic microvascular oscillations (choledocic
and/or upper and low ureteral reflexes) show the most intense degree,
almost equal to that of the highest spikes (HS), demonstrating
clearly the real biological nature of oscillating complexity, namely the
adaptative capacity and ability to responde. In
fact, during phlogistic process, the interstitial oedema increases both
vasomotility and vasomotion, as experimental evidence demonstrates (=
occlusive digital pressure upon superficial lymphatic vessels) (22).
In other words, chaos theory has stimulated some important
technical developments in the way we can analyze and interpret medical
and other time series data (23). As
regards the above-mentioned "strange attractors" of chaotic
dynamic systems, a key concept is "fractal dimension", very
different from the topological one, as demonstrates the generation of
Koch's curve (24), which, as the name implies, was developed for
fractals, but the practical applications of which has emerged as a
byproduct of attempts to prove that certain systems have strange,
chaotic, fractal at-tractors, by analyzing time evolution data (23). When
brain wave data, e.g., in rats are "re-constructed", the
attractor for a healthy rat is computed to have a "dimension"
of about 5,9 while that for the same rat in epileptic seizure has a
dimension of only 2,5 (25). The suggestion is that the "dimension"
correlates with the flexibility and adaptability of the
organisms: the larger number implies a chaotic system with well
developed flexible response to stimuli, whereas the low value associated
with the seizure can be regarded as evidence of suppression or
malfunction of a number of key elements of the rat's physiology. A
somewhat similar argument can be applied to biophysical-semeiotic data,
as regards, e.g., pancreatic oscillations in case of classical or "variant"
Reaven's syndrome in diabetic evolution (26) as well as in diabetes
mellitus (22). It must also be remembered that fractal dimension (fD)
and system complexity are directly correlated. From
the above remarks, there is chaos in the microvascular system (See my
site http://digilander.libero.it/microangiologia).
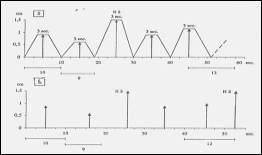
In
facts, intensity of choledocic and low ureteral reflexes is really
different in the healthy subjects, as the reflex oscillation is
concerned, varying from 0,5 to 1,5 cm, from biophysical semeiotic
stand-point, so that the ratio HS/minimal fluctuations is 3/1. The
oscillations become less chaotic when an organ is evolving to a
pathological state and finally all oscillations are identical and
regular in diseased organs: f D decreases from 3,81
(NN = 3,81) to 1. Analogously,
we observe deterministic chaos in the duration of single cycle; the
lenght of normal period is 10,5 sec in an average, ranging from 9 to 12
sec. In hyperfunctioning organs, e.g. in case of a trivial flu, as bone
marrow is concerned for example, oscillation intensity is like HS and
cycle duration results restricted to 9-11 sec. On the other hand, in
diseased organ the duration is fixed at 10 sec. and intensity is 0,5 cm.
The
clinical evidence corroborates biophysical semeiotic theory of the
existence of chaos in microcirculatory bed because there is a perfect
concordance between chaos and biophysical semeiotic parameters. Our
clinical biophysical semeiotic data corroborate actually those of other
A. (27, 28), about random, chaotic activity in the “vasomotion”, due
to the great number of different in-put in the smooth muscle cells. In
diseased organ it is possible that a lot of in-puts decrease and/or
disappear and a mechanism becomes dominant. Consequently the tissue
present rhythmic “vasomotion” (25, 29), as demonstrated in our
tachograms (See later on). In
case of "pathological" oedema, a lot of stimuli, which bring
about a random, chaotic “vasomotion”, apparently are eliminated,
causing a regular “vasomotion” (25, 29), as we observed in a long,
well established experience. On the contrary, in a jatrogenic oedema,
i.e. during digital lymphatic or venous vessels obstruction, after 2 sec
vasomotility increases, showing exclusively HS and, therafter, also
vasomotion becomes very intense. From
the above remarks, the vasomotion clearly depends from vasomotility and
the two phenomena are really different in nature (22, 30). Due
to a lot of in-puts small arteries and arterioles constrict and dilate
autonomously (6 cycles per minute, from biophysical semeiotic
stand-point), as arteriolar choledocic reflex demonstrates, because of
numerous arteriolar pace-makers. This arteriolar vasomotility, based on
sphygmicity, aimes at maintaining a physiological “vasomotion” and
consequently flow-motion, so that O2 and metabolites tissue
supply persists normal under different conditions. Therefore, vascular
tone and vasomotility of healthy people are in perfect relation to
tissue request. In
an organ or tissue, in other words, arteriolar activity and diameter are
generally correlated to a certain extence. Under physiological
conditions, arteriolar tone enhancing brings about increasing of blood
pressure. In such case, due to secondary hypoxia, the blood pressure
should subsequently increase (30). On the contrary, the increased
vasomotility, due to enhanced tone, permits to maintaining a regular
flow-motion and fuell supplying, although high blood pressure as well as
hematocryt, avoiding a vicious circle. From
a physiological point of view, vasomotility and vasomotion provide to: 1)
efficacious and economic tissue blood distribution; 2) reducing peripheral vascular resistence; 3)
under
some circumstances, permits interstitial fluid to be absorbed (28, 31). Interestingly,
Biophysical Semeiotics allows the doctor to observe clinical and
experimental evidence, which enlights the relation between vasomotility
and vasomotion: digital pressure upon radial arteries induces down-wards
in succession arteriolar dilation with increased vasomotility ®
enhancing of vasomotion ®
occlusion (disactivation) of AVA, functionally speaking, so that O2
and metabolites supply to tissues persists in normal ranges to certain
extence of digital pressure. From
the above remarks, one can understand that, in case of essential
hypertension, e.g., the used drug results really efficacious exclusively
in the case fractal dimension of resistence microvessels returnes to
physiological values, beside the normalization of blood pressure. At
this point I illustrate an interesting aspect of vasomotion, wich allows
readers to understand the primary role played by microcircle
abnormalities in the oncogenesis. Biophysical-Semeiotic
morphological analysis of vasomotion in both physiology and pathology. From
the practical point of view it is sufficient and reliable to evaluate
periods as well as intensity of low ureteral reflex oscillation (=
vasomotion), as described above, for example during mean digital
pressure, applied upon the middle third of biceps muscle, compressing it
between thumb and other fingers, of a supine individual,
psychophysically relaxed. The muscle pressure allows doctor to examine
resistance microvessels dynamics and flowmotion of nutritional
capillaries. However,
the original morphological analysis of vasomotion, i.e the precise
evaluation of low ureteral reflex oscillations, reveals interestingly
the actual condition of related tissue-micro vascular-units, in whatever
tissue, in a synergetic model. In order to realize this analysis is
unavoidable to transfer upon Cartesian coordinates intensity (ordinate,
cm) and duration (abscisse, sec.) of three successive fluctuations of
low ureteral reflex, observed for example in the above-mentioned
situation, during biceps muscle microvascular units stimulation. In
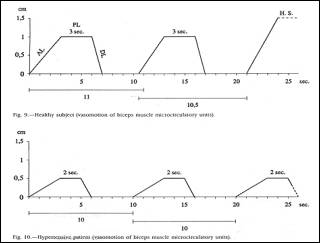
healthy subject we observe a characteristic diagram (Fig. 1).
Fig.
1 Interestingly,
in 3 sec (ascending line: AL) it is reached the highest intensity (NN =
0,5-1,5 cm); the "plateau" line (PL) lasts physiologically 3
sec, then in 1 sec (descending line: DL) the line returns to basal value
(i.e. abscisse), where persists for 2-5 sec, varying the periods from 9
to 12 seconds under physiological condition. On
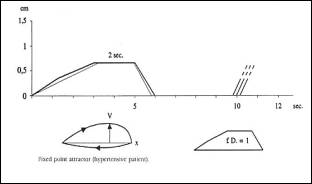
the contrary, in pathological situations, e.g. essential hypertension,
the diagram results interestingly modified (Fig.2): AL as well as DL are
normal, 3 sec. and 1 sec respectively; intensity is approxi-mately 0,5
cm, in a "predictable" manner; the physiological highest waves,
i.e. highest spikes of 1.5 cm intensity (HS), are absent.
Fig.2 In
the figure are referred, in geometrical manner, the physiological
microcirculation of biceps muscle (oben) and that of an hypertensive
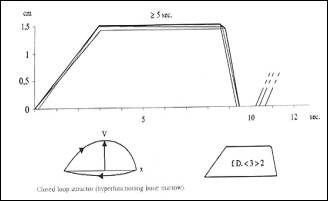
patient. Finally,
in case of hyperfunctioning tissue, e.g. the bone-marrow during
infective disorders of whatever nature, digital pressure upon the middle
line of breast bone, brings about low ureteral reflex oscillations,
characterized by PL of 5 or more sec, intensity as well as periods
practically identical each other (Fig. 3). Intensity and PL of every
oscillation are directly correlated: more high the intensity, more
prolonged appears PL and consequently more efficacious is the
flow-motion of related nutritional capillaries.
Fig.
3 Vasomotion
of hyperfunctioning tissue-microvascular unit(e.g. bone marrow). This
clinical evidence underlines the inner consistence of Biophysical
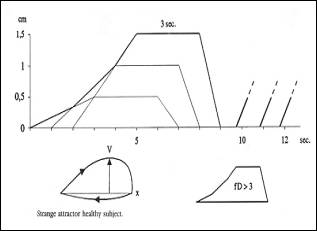
Semeiotics. In
addition, superimposing the parameters of three subsequent oscillations
of low ureteral reflex, in accordance with the lenght of single period,
we realize really interesting figures. In healthy people the obtained
area shows a "strange" shape, like a "strange"
attractor (Fig. 4: fractal dimension (fD) >3 (22), that corresponds
to the space occupied by a fractal structure.
Fig.
4 Strange
attractor: healthy subject. On
the contrary, under pathological condition, e.g. essential hypertension
as far as biceps muscle microcirculatory bed is concerned, the area
obtained in this manner appears quite small, resembling an attractor at
fixed point (Fig. 5).
Fig.
5 Fixed
point attractor: hypertensive patient Finally,
the area corresponding to hyperfunctioning microcirculatory units
results the largest one, due exclusively to its large Euclidean
perimeter; its shape, however, resembles clearly a deformed circle,
corresponding to a “closed loop” attractor (Fig. 6) (32, 33).
Fig.
6 Closed
loop attractor in hyperfunctioning bone-marrow. From
the above remarks it results that morphological analysis of vasomotion,
by means of Biophysical Semeiotics, in physiological as well as
in pathological conditions, represents an original, reliable and usefull
tool in both clinics and research, as allows us to state a long, well
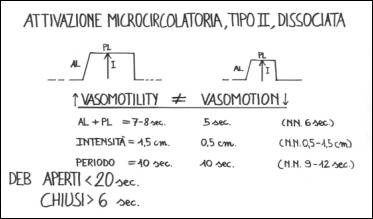
established experience. We
can now turn to our argument, saying that in the precise site of
real risk for breast cancer, “light” digital
pressure causes upper (= vasomotility) and lower (vasomotion) ureteral
reflexes, which show the characteristic type II, dissociated
microcirculatory activation: at rest, upper ureteral reflex oscillations
last 7-8 sec. (NN = 6 sec.), in relation to the seriousness of
underlying risk, while lower ureteral reflex fluctuates for 6 sec., i.e.
normally, (or less than normally, in particularly serious cases),
although related vasomotility is increased (Fig. 7). Consequently,
doctor can recognize the precise site as well as “quantify” the real
risk for breast and
other cancer, thanks the modified microcirculatory activity, which
appears more clearly altered under stress tests, as boxer’s test,
apnea test, Restano’s manoeuvre, insulin secretion acute pick test,
a.s.o. (See Glossary in the above-cited site).
Fig.
7 The
figure shows, in
geometrical manner, the characteristic oscillations
of upper (vasomotility) and lower (vasomotion) ureteral reflexes,
during small stimulation of the trigger-points, precisely
related to diseased tissular area, in case of type II,
dissociated, microcirculatory activation. Doctor can
observe as well as quantify
them, of course, generally in individual, apparently healthy, but
really involved by
oncological terrain and at
real risk for cancer, different in intensity,
in whatever biological system. 1) Watts G. Three cell cycle scientists win Nobel prize. BMJ 2001; 323:823 (13 October). 2) Stagnaro-Neri M., Stagnaro S., Semeiotica Biofisica del torace, della circolazione ematica e dell’anticorpopoiesi acuta e cronica. Acta Med. Medit. 13, 25 1997 3) Stagnaro-Neri M., Stagnaro S., Semeiotica Biofisica: la manovra di Ferrero-Marigo nella diagnosi clinica della iperinsulinemia-insulino resistenza. Acta Med. Medit. 13, 125 1997 4) Stagnaro-Neri
M., Stagnaro S., Cancro della mammella: prevenzione primaria e diagnosi
precoce con la percussione ascoltata. Gazz. Med. It. – Arch.
Sc. Med. 152, 447,
1993. 5)
Stagnaro S., Diet and Risk of Type 2 Diabetes. N Engl J Med. 2002 Jan 24;346(4):297-298. letter [PubMed
–indexed for MEDLINE]. 6) Cortez
D, Wang Y, Qin J, Elledge SJ. Requirement
of ATM-dependent phosphorylation of brca1 in the DNA damage response to
double-strand breaks. Science 1999;286:1162-6. 7)
Li S, Ting NSY, Zheng L, et al. Functionallink ofBRCA1 and ataxia
telangiectasia gene product in DNA damage response. Nature 2000;406:
210-5. 8)
Bell DW, Vatley JM, Szydlo TE, et al. Heterozygous germ line hCHK2
mutations in Li-Fraumeni syndrome. Science
1999;286:2528-31. 9)
Hirao, A, Kong, Y-Y, Matsuoka S, et al. DNA damage-induced activa- tion ofp53 by the checkpoint kinase Chk2.
Science 2000;287:1824-7. 10)
Zhao S, Weng Y-C, Yuan S-S, et al. Functionallink between
ataxia-telangiectasia and Nijmegen breakage syndrome gene products.
Nature 2000; 405:473-7. 11)
Wu X, Ranganathan V, Weisman DS, et al. ATM phosphorylation of Nijmegen
breakage syndrome protein is reqnired in a DNA damage response. Nature
2000;405:477-82. 12)
Lee J-S, Collins KM, Brown AL, Lee C-H, Chung JH. hCds1-Mediated
phosphorylation of BRCA1 regulates the DNA damage response. Nature
2000;404:201-4. 13)
Wang Y, Cortez D, Yazdi P, NeffN, Elledge SJ, Qin J. BASC, a super
complex of BRCA1-associated proteins involved in the recognition and
repair of aberrant DNA structures. Genes Dev 2000;14:927-39. 14)
Swift M, Morrell D, Massey RB, Chase CL. Incidence of cancer in 161
families affected by ataxia-telangiectasia. N Engl J Med
1991;325:1831-6. 15)
FitzGerald MG, Bean JM, Hegde SR, et al. Heterozygous
ATM mutations do not contribute to early onset of breast cancer. Nat
Genet 1997; 15:307-10. 16)
Dorozynski
A. Chaos. Br Med J 1989;298:350-1. 17)
Goldberger AL, Lipsitz LA. Andamenti frattalici e rigidità patologiche.
Sfera. Editrice Sigma Tau, n 36:62-5. 18)
Stagnaro-Neri M, Stagnaro S. Aritmia splenica, segno attendibile di
patologia bilio-duodenale. Minerva Med, 1985;76:30-1 [Pub-Med
indexed for Medline]. 19) Stagnaro-Neri M. Stagnaro S. Ketanserina, antagonista dei recettori 5 HT-2-serotoninergici e scavenger dei radicali liberi epatici. Clin Ter l992;l4l:465-73 [Pub-Med indexed for Medline]. 20)
Stagnaro-Neri M, Stagnaro S.
Valutazione percusso-ascoltatoria del sistema nervoso vegetative e del
sistema renina angiotensina, circolante e tessutale. Arch Med Int 1992;3:173-92. 21) Stagnaro-Neri M,
Stagnaro S. Aritmia splenica, segno attendibile di patologia
bilio-duodenale. Minerva Med, 1985;76:30-1 [Pub-Med
indexed for Medline]. 22) Stagnaro-Neri M, Stagnaro S. Vasomotility e Vasomotion nelle flebopatie ipotoniche istangiopatiche: caos deterministico e unita microvascolotessutale. Comun.Congresso Naz Soc It Flebologia Clin e Speriment, Catania, 4-7/12/1993. 23)
Firth WJ. Chaos—predicting the unpredictable.
Br Med J 1991;303:1565-8. 24)
Glenny RW, Robertson AT. Fractal properties of pulmonary blood flow:
characterization of spatial heterogeneity. Am Physiol Soc 1990:531-45. 25)
Freeman WJ. Strange attractors that govern mammalian brain dynamics
shown by trajectories of electroencephalographic (EEG) potential.
Transaction on circuits and
systems. Brain, 1988;35:781-4. 26) Stagnaro-Neri M,
Stagnaro S. Sindrome di Reaven, classica e variante, in evoluzione
diabetica. II ruolo della carnitina nella prevenzione primaria del
diabete mellito. II Cuore 1993;6:6l7-24. [Pub-Med
indexed for Medline]. 27) Intaglietta M,
Allegra C. Vasomotion and flowmotion. Minerva Angiol 1992;17 (Suppl 2 al
N 2):215-8. 28) Intaglietta M, Breit
GA. Vasomotor activity. In: Progress in applied
microcirculation. Basel:
Karger, 1988:25-32. 29)
Intaglietta M, Allegra C. Vasomotion and flowmotion. Minerva
Angiol 1992;17 (Suppl 2 al N 2):215-8. 30) Curri SB. Rapporti
tra vasomotilita, periangio, sostanza fondamentale del connettivo e
linfatici. Minerva Angiol 1992;17(Suppl 2 al N 2):181-9. 31)
Folkow B. Description of the myogenic hypothesis. Circulat Res 1964;l4-15(Suppl):1279-85. 32) Peitgen HO, Richter
PH. La bellezza dei frattali. Immagini di sistemi dinamici complessi.
Torino: Ed Bollati Boringhieri, 1991. 33)
Ruelle D. Caso e caos. Torino: Ed Bollati Boringhieri, 1992. 34) Stagnaro-Neri M,
Stagnaro S. Cancro della mammella: prevenzione primaria e diagnosi
clinica precoce con la percussione ascoltata. Gazz
Med It - Arch Sci Med 35) Peters MA., Stanford
JL., Badzioch MD., et al. Genome-wide
scan for high-risk prostate cancer families with breast cancer reveals
new loci for prostate cancer and breast cancer. Nature Genetics 36) Thompson D., Easton D.F. Cancer Incidence in BRCA1 Mutation Carriers. Journal of the National Cancer Institute, Vol. 94, No. 18, 1358-1365, September 18, 2002 Last update: March 18, 2018 |